

Trauma
A 29 year old rugby player presents to the Emergency Department complaining of pain in the left wrist following a fall the same day. On examination you note tenderness in the anatomical snuffbox on palpation and on telescoping the thumb. An x-ray is performed and you cannot see a bony injury. How should this patient be managed?
Answer:
If a scaphoid fracture is clinically suspected but no fracture is visible on radiographs:- Immobilise the wrist in a splint
- Inform the patient that a significant fracture may still be present
- Refer to a specialist clinic or directly for MRI, if locally available
Scaphoid Fracture and Other Carpal Injuries
Trauma
Last Updated: 24th February 2026
Clinical anatomy

Carpal Bones. (Image by Dr. Jochen Lengerke at de.wikipedia. Painted color by User:Was a bee. (File:Xray hand.jpg) [Public domain], via Wikimedia Commons)
- Proximal row
- A: Scaphoid
- B: Lunate
- C: Triquetrum
- D: Pisiform
- Distal row:
- E: Trapezium
- F: Trapezoid
- G: Capitate
- H: Hamate
Anatomical snuffbox borders:
- Ulnar border – tendon of the extensor pollicis longus
- Radial border – tendon of the abductor pollicis longus and extensor pollicis brevis
- Proximal border – styloid process of the radius
- Distal border – base of thumb metacarpal
- Floor – carpal bones; scaphoid and trapezium
- Roof – skin
Anatomical snuffbox contents:
- Radial artery
- Branch of the radial nerve
- Cephalic vein
Scaphoid fracture
When to Suspect a Scaphoid Fracture
Scaphoid fractures most commonly occur in young men, but they can occur at any age and in either sex.
A scaphoid fracture should be suspected following:
- A forced hyperextension injury to the wrist (e.g. fall on an outstretched hand, football save)
- A punching injury
- Major wrist trauma
AND the presence of at least one of the following:
- Scaphoid tenderness:
- Anatomical snuffbox (ASB)
- Proximal pole
- Tuberosity
- Pain in the anatomical snuffbox on active ulnar deviation
- Pain on axial loading of the thumb
ED Management
If a scaphoid fracture is suspected, request at least four radiographic views:
- Posteroanterior (PA)
- Lateral
- Semi-prone
- Elongated scaphoid view
If plain radiographs confirm a scaphoid fracture:
- Apply a below-elbow plaster backslab
- Refer to a specialist clinic
- Specialist review should occur within 7–14 days
Fractures displaced > 2 mm must be assessed carefully to exclude a perilunate injury and referred urgently for specialist opinion.
If a scaphoid fracture is clinically suspected but no fracture is visible on radiographs:
- Immobilise the wrist in a splint
- Inform the patient that a significant fracture may still be present
- Refer to a specialist clinic or directly for MRI, if locally available
Specialist Management
- If referrals are reviewed in a virtual clinic, patients may be referred directly for MRI for a suspected scaphoid fracture (if considered high risk) or CT for a definite fracture. Other patients with a suspected fracture should receive an appointment within 1 week for clinical assessment. Alternatively, patients may receive an information leaflet and patient-initiated follow-up, if a local policy for this exists.
- A definitive management plan for patients with a suspected scaphoid fracture should be in place within 2 weeks of presentation. This should include MRI or CT to exclude a fracture unless there is a clear alternative diagnosis. MRI is the recommended imaging modality.
- If a scaphoid fracture is visible on plain radiographs, CT scan should be performed to measure displacement accurately. Reconstructions should be performed in the sagittal and coronal planes with respect to the long axis of the scaphoid.
- Scaphoid waist fractures with <2mm displacement or distal pole fractures can be treated by immobilisation in a below elbow cast with the thumb excluded.
- Scaphoid tuberosity avulsion fractures can be treated with immobilisation for 4-6 weeks as required for symptom control.
- The following are indications for acute surgical fixation, which should be ideally performed within 2 weeks of injury:
- a) Fractures of the scaphoid waist with >2mm displacement6
- b) Fractures associated with an unstable carpal injury or displaced distal radial
fracture - c) Fractures of the proximal pole with any displacement
- Patients with a delay in immobilisation of more than 4 weeks for a minimally displaced waist fracture should be referred for CT to assess union and be considered for surgical fixation if there is no evidence of union.
- Patients managed non-operatively should have radiographs (out of cast) or CT scan by 6-8 weeks post injury. Patients who have scaphoid tenderness and no progression of union on radiographs at 6 weeks or who develop cystic change at any stage should be investigated by CT. If this demonstrates a clear fracture gap and no evidence of union, consider surgical fixation +/-bone grafting within 2 weeks. If there are early signs of union, continue wrist immobilisation and review at 12 weeks with plain radiographs and CT if radiographs are equivocal. Patients with any evidence of non-union at this time should be offered surgery, if treatment is appropriate.
- Patients should only be discharged once union is confirmed on CT (>50% of the fracture cross-sectional area) or by delayed radiographs at 6 months. All patients should be advised of the small ongoing risk of non-union and that they must return for further assessment if symptoms develop.
Complications
It is important to appreciate the blood supply to the scaphoid, which is by branches of the radial artery. The dorsal branch of the radial artery, which supplies 80% of the blood, enters in the distal pole and travels in a retrograde fashion towards the proximal pole. Consequently, fractures can compromise the blood supply, leading to avascular necrosis (AVN) and subsequent degenerative wrist disease. The more proximal the scaphoid fracture, the higher the risk of AVN.
Non-union is the bone failing to heal properly, most commonly due to a poor blood supply. It is particularly common in scaphoid fractures that go undiagnosed or are inappropriately managed.
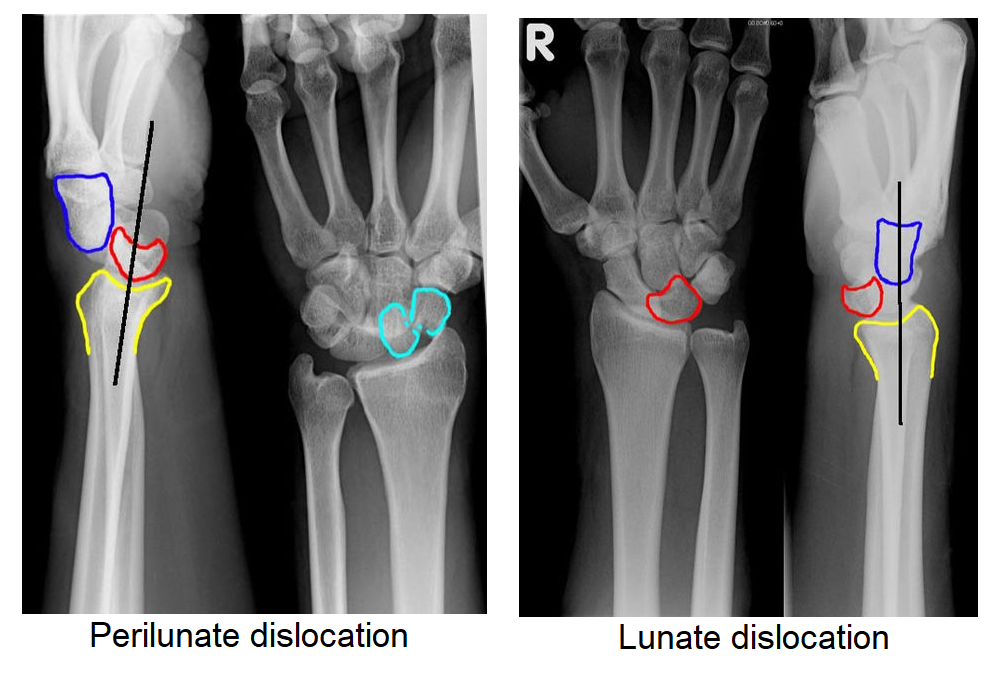
Lunate and perilunate dislocations
- Definition:
- Perilunate Dislocation = Lunate stays in place, capitate is displaced
- Lunate Dislocation = Capitate stays in place, lunate is displaced
- Background:
- Typically occur via high-energy FOOSH injury (fall from height, RTC)
- Commonly missed (~25%) on initial presentation
- Must rule-out median nerve injury
- Must rule out carpal bone fractures
- Clinical features:
- Perilunate dislocation: dorsal swelling with palpable mass
- Lunate dislocation: volar swelling with palpable mass
- X-ray:
- Perilunate dislocation:
- Lateral view: Capitate is displaced dorsal to lunate and lunate retains its normal contact with radius
- PA view: Capitolunate joint space is obliterated as the bones overlap one another
- Lunate dislocation:
- Lateral view: Lunate is pushed off the radius into the palm ("spilled teacup" sign)
- PA view: Lunate has triangular shape ("piece-of-pie sign")
- Perilunate dislocation:
- Management:
- Closed reduction and long-arm splint
- Requires emergent ortho consultation (very difficult to reduce with high incidence of median nerve compression), and usually emergent operative management
Other carpal injuries
- Fractured hook of the hamate
- Local palmar tenderness may give rise to suspicion of a fracture of the hook of the hamate.
- Diagnosis can be difficult— specialised X- rays or CT may be required to demonstrate the fracture.
- Immobilise in POP and refer to the fracture clinic.
- Flake avulsion carpal fractures
- Small avulsions from the dorsum of the carpus are often from the triquetrum.
- Treat with immobilisation in a POP backslab or a wrist support splint and analgesia, and refer to the fracture clinic.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |