

Ophthalmology
A 15 year old boy presents to the ED after having been shot in the face with a BB gun. He has a solitary penetrating wound just inferior to his left eye. His visual acuity in the left eye is limited to light perception, but he reports having normal vision prior to the injury. He has significant proptosis of his left eye, and his fundus is clearly seen with direct ophthalmoscopy. Intraocular pressure (IOP) of the affected eye is 50 mmHg. His mental status is normal. What is the most appropriate next step in the management of this patient?
Answer:
The described patient likely has a retrobulbar haematoma with visual acuity changes and an elevated IOP. The elevated IOP with a clear funduscopy are findings consistent with no penetration into the globe. Although CT scan of the head and face is indicated to further delineate specific injuries, lateral canthotomy and inferior cantholysis is emergently necessary for orbital decompression in an attempt to salvage visual function. This sight-saving procedure should not be delayed more than 2 hours after injury when severe findings (decreased visual acuity and significantly increased IOP) are present. Likewise, ophthalmology consultation would be indicated emergently. Plain films of the face would prove of little use in the evaluation of this patient, as would prolonged ED observation.Eye Trauma
Ophthalmology
Last Updated: 16th July 2025
Anatomy of the eye
- The cornea is the transparent layer that forms the anterior boundary of the space known as the anterior chamber, and it is contiguous with the sclera.
- The interior of the globe is divided into anterior and posterior segments by the lens.
- The anterior segment includes the cornea, sclera, conjunctiva, iris, and lens. The space between the cornea and iris is called the anterior chamber and is filled with aqueous humor.
- The posterior segment of the globe is between the lens and the retina, and it is filled with vitreous humor.
- The optic nerve is at the back of the eye; it travels through the muscle cone, through the orbit, and then into the brain.
- The sclera and extraocular muscles are covered by an epithelium called the conjunctiva, which extends from the cornea-sclera junction over the sclera and then turns to cover the inside of the eyelids.
- The extraocular muscles join together to make a “cone,” which is covered in a fascia-like sheath called Tenon’s capsule. This minimally distensible fascial covering limits the ability of these muscles to expand; thus, haemorrhage in this area may produce a compartment syndrome.
- The globe–muscle cone complex sits in the orbit of the eye, which is a pear-shaped cavity formed by bones that separate the orbital compartment from the sinus and brain tissue.
- The eyelids have tendinous attachments (canthal tendons) medially and temporally on the bony orbit, which keep the globe from moving forward. This arrangement creates another space with limited expansion where compartment syndrome can also occur.
- The nasal portion of the upper and lower eyelids contains the superior and inferior puncta and canaliculi, which drain tears from the ocular surface. Tears flow through the puncta, then through the canaliculi into the lacrimal sac and then down the nasolacrimal duct into the nose.
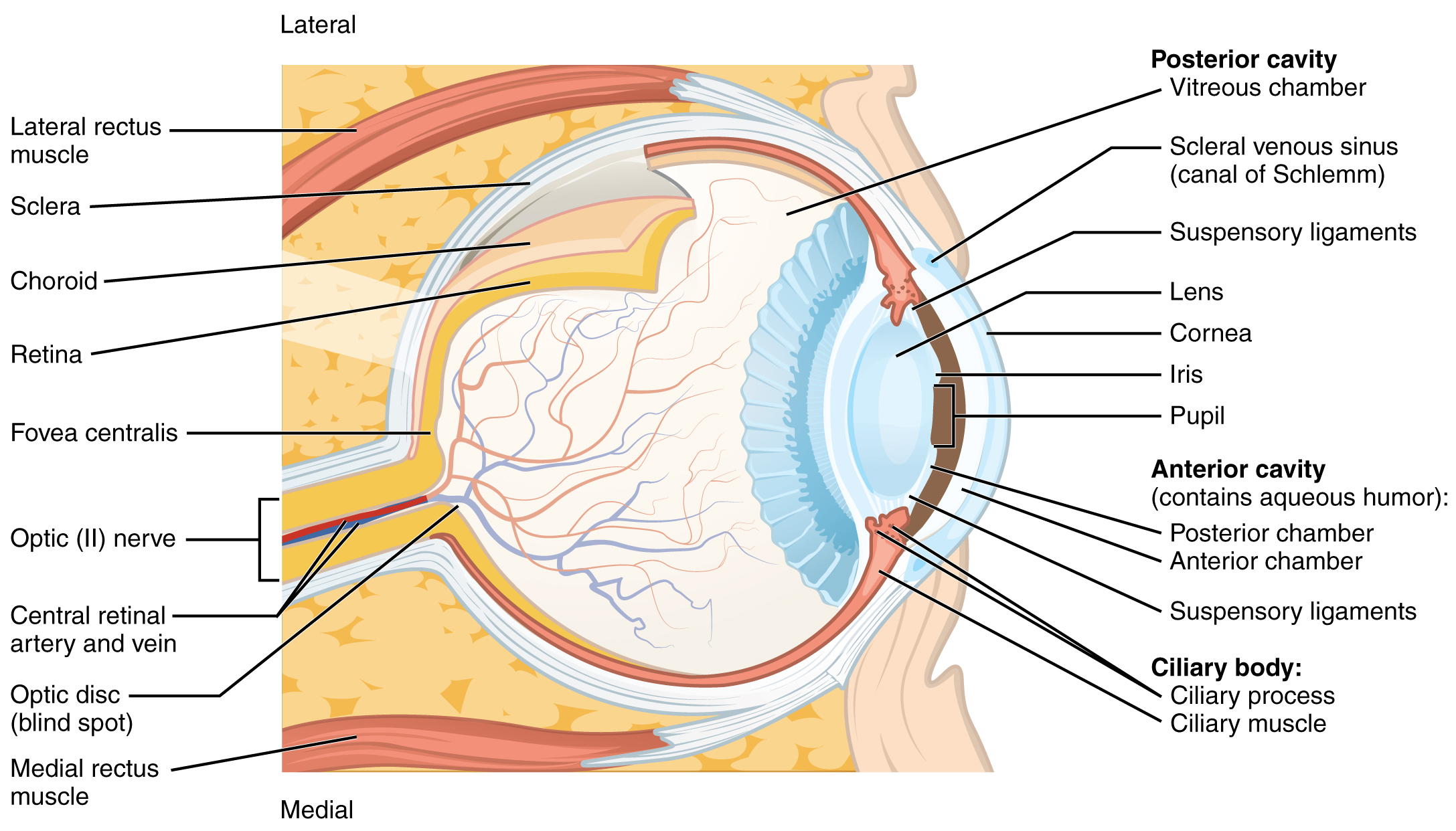
Anatomy of the Eye. (Image by OpenStax College [CC BY (https://creativecommons.org/licenses/by/3.0)])
Assessment of the eye
Vision
- A vision exam can be as simple as holding up a near vision test card or any reading material at the appropriate distance and recording the vision in each eye.
- Always note if the patient normally wears glasses or contact lenses, and if so, whether for distance or near (reading) vision. If a refractive error is known, but the patient does not have glasses, ask the patient to look through a pinhole, which minimises the refractive error, and recheck the vision.
Pupils
- Pupils should be equal, round, reactive and without an afferent pupillary defect. A sluggish or poorly reactive pupil indicates a possible brain abnormality such as stroke or herniation. Be aware that these findings do not typically indicate ocular pathology.
- However, it is important to note that a pupil can become enlarged due to blunt trauma (e.g. pupillary sphincter tear), past surgery, and other ocular disease processes. When an abnormal pupillary exam results from an ocular cause alone, the pupil often retains some reactivity to light, even though it is a different size. The patient’s medical history should reflect a positive past ocular history; if it does not, further investigation and examination is necessary to evaluate for intracranial pathology.
- In checking for optic nerve dysfunction, use the “swinging flashlight test” to look for an afferent pupillary defect. When there is concern for optic nerve dysfunction related to trauma, consult an ophthalmologist for a detailed examination.
Intraocular pressure
- Handheld tonometry devices, such as the Tono-pen, are now available in many emergency rooms. These gauges have improved the clinician’s ability to check eye pressures in diverse patient situations. When using handheld tonometry devices, open the eyelid while being careful not to push on the globe, because doing so can falsely elevate the eye pressure. Make sure the fingers retracting the eyelids are resting on the bony orbit, not the globe. Always obtain 2–3 measurements of each eye, at the highest percentage of reliability on the Tono-pen (normal eye pressure is between 8 and 21 mmHg). The “data” or “%” reading on the pen indicates the likelihood that this reading is accurate. It is important to note that readings can vary with mechanical ventilation, Valsalva maneuvers, and accidental pressure on the globe during eye opening.
- When possible, anaesthetise the eye with topical anesthetic ophthalmic drops if the patient is not fully sedated. Otherwise, the patient may blink excessively or squeeze the eyelids shut when the tip of the instrument touches the eye.
- Without a tonometer, you can roughly estimate eye pressure by gently pressing with two index fingers on each side of the eye with the eyelids closed. If you are unsure what normal is, press your own eye or the patient’s unaffected eye in the same manner and compare. Most importantly, evaluate whether the patient has a firmer eye on the injured side.
- If an open globe is suspected, do not check the eye pressure, because you might drive more intraocular contents from the eye. In such cases, check visual acuity and conduct a visual inspection only
Anterior exam
The anterior exam addresses several aspects of eye anatomy: the periorbita, extraocular muscles, lids, lashes, lacrimal sacs, conjunctiva, sclera, cornea, iris, anterior chamber, and lens.
- Periorbita:
- Note any ecchymosis and lacerations around the eye.
- Evaluate the forward extent of the globes. This can be done with eyelids open or closed, by looking down the face while the patient is supine and determining if one eye is farther forward than the other. This can also be evaluated radiographically by using the axial cut of a CT head scan through the orbits, measuring from the lateral wall of the orbit to the nose on each side, and then determining how much of the globe protrudes beyond this imaginary line.
- On a normal exam, when you gently push on the eye through the eyelid, you will feel the globe give a little and move backward. When this does not occur, there is resistance to retropulsion, indicating the possibility of increased pressure behind the eye, as with a retrobulbar haemorrhage. Another sign of retrobulbar haemorrhage is when the globe pushes against the eyelids, creating such pressure that the eyelid is taut and cannot be pulled away from the globe.
- Lastly, when evaluating wounds of the periorbita, always inspect lacerations to ensure they are not full thickness and eliminate the possibility of a concealed foreign body. Even if the globe seems unaffected, any foreign bodies penetrating the orbit require immediate ophthalmic examination to determine if the globe is open.
- Extraocular muscles:
- For patients able to follow instructions, ask them to follow your finger up, down, and side to side.
- Restricted ocular movement may be from high pressure inside the orbit, from orbital fractures, or from muscle or nerve injury.
- Lids, lashes, and lacrimal sac:
- Examine the eyelids to look for lacerations, and note whether they are full or partial thickness. Full-thickness lid lacerations require surgical repair by a surgeon familiar with eyelid and lacrimal drainage anatomy. Although this procedure need not happen immediately, repair within 72 hours of injury increases the likelihood of success. If the nasolacrimal duct system is involved, it is most ideal to repair before onset of tissue oedema, so consult a specialist as soon as you identify the issue.
- Be especially aware of eyelid lacerations that align with conjunctival or corneal lacerations, because these are often associated with occult open globes.
- Conjunctiva, sclera, and cornea:
- Note any subconjunctival haemorrhages and their extent; the more extensive they are, the more likely the globe itself has sustained substantial injuries.
- If the conjunctiva is lacerated, pay close attention to the underlying sclera, which may also be lacerated. Again, an injury like this could indicate an occult open globe.
- Also check for lacerations or abrasions of the conjunctiva, sclera, and cornea, noting their relationship to any eyelid lacerations.
- To check for subtle injuries of the conjunctiva and cornea, conduct the fluorescein dye test:
- Anaesthetise the eye with topical drops.
- Using a moistened fluorescein strip, place a few drops of fluorescein in the eye. (The patient may need to blink to fully distribute the dye.)
- Shine a blue light (Wood’s lamp or ophthalmoscope) on the eye.
- The dye will fluoresce in the green spectrum and highlight the area of epithelium that has been disrupted.
- Abrasions of the cornea or conjunctiva can be treated with simple ophthalmic ointment. Lacerations of the cornea or sclera are of greater concern because when full thickness, they indicate an open globe. This injury requires immediate consultation with an ophthalmologist for further evaluation.
- Lastly, if you note that the patient is wearing contact lenses; remove them, as wearing contact lenses for an extended period of time greatly increases the risk of infectious corneal ulcers. The fluorescein dye test may also be helpful in identifying infectious corneal ulcers and occult open globes.
- Iris:
- The iris is a spongy, distensible muscle that is generally round and reactive to light. If the pupil is round and reactive to light, but slightly larger than the pupil of the unaffected eye, the patient likely has a pupillary sphincter tear. This injury commonly occurs with blunt trauma to the globe.
- However, if the pupil is not round, further examination is warranted. With smaller globe injuries, the globe may remain formed, but the pupil will have an irregular “peaked” appearance. Look for the iris plugging the hole in the globe or poking out of the sclera or cornea in the direction in which the peaked pupil is pointing: This is where the full-thickness corneal or scleral laceration should be.
- Anterior chamber:
- The anterior chamber should be relatively deep; i.e. the iris should be flat with an approximately 45-degree angle between the iris plane and the curve of the cornea, and be full of clear, aqueous humor. When the iris is close to the cornea, or the anterior chamber is “shallow,” aqueous humor may be leaking out due to an open globe. Look closely for clouding of this fluid, which may indicate the presence of red blood cells.
- Blood in the anterior chamber, known as a hyphaema, has two forms:
- (1) dispersed, with red blood cells floating in the aqueous humor and thus making the patient’s vision and your view into the eye hazy
- (2) layered, with blood on top of the iris; or layered, with blood inferiorly if gravity has shifted the blood cells down
- A hyphaema may cause dramatically elevated intraocular pressure and can indicate significant trauma to the globe. It is important to consult an ophthalmologist immediately if this diagnosis is made.
- Lens:
- The lens is typically clear in young people or appears varying shades of yellow in patients older than 40 years (e.g. indicating a cataract).
- The lens is encased in a clear, taut capsule. If the capsule is violated, the lens turns white, often swelling with time. This injury can induce significant intraocular inflammation and elevated intraocular pressure, unless there is a concomitant large globe injury. If the examination indicates a violated lens capsule, the globe is most likely open, and the eye may contain a foreign body.
Posterior exam
- The posterior segment eye exam can be difficult, especially if the pupil is small due to sedatives or pain medications. You can usually observe the presence of a red reflex (i.e. reddish orange reflection of light from the retina) at a minimum.
- If the pupil is larger, you can use an ophthalmoscope to visualise the optic nerve and/or posterior retina, but this is still not a complete exam. If you cannot view the back of the eye, you cannot exclude the possibility of vitreous haemorrhage, retinal detachment, or other pathology.
- Unlike spontaneous retinal detachments, traumatic retinal detachments or other posterior pathology is not usually treated with emergent surgery. Nevertheless, be sure to notify the ophthalmologist on call of your findings because vitreous haemorrhage from trauma is usually a result of significant force and the eye is at risk for more serious injuries.
Specific ocular injuries
Orbit fractures and retrobulbar haemorrhages
- Fractures of the orbit may cause bleeding in the muscle cone or around it. These compartments are limited by the insertion of the eyelid tendons to the bony attachments of the medial and lateral canthi. If the bleeding is significant enough, a compartment syndrome can develop that obstructs the blood supply to the optic nerve and globe.
- Signs of a retrobulbar haemorrhage with compartment syndrome include decreased vision, elevated eye pressure, asymmetrical proptosis (eye bulge), resistance to retropulsion, and tight eyelids against the globe. A CT scan can reveal retrobulbar haemorrhage, but only a clinical exam will determine whether this bleeding is causing a compartment syndrome and requires treatment. Vision loss can occur after about 1.5 hours of impaired blood supply, so immediate treatment is imperative.
- If you are concerned about a retrobulbar haemorrhage causing a compartment syndrome, immediately contact a provider who has the ability to perform canthotomy and cantholysis. Canthotomy alone (i.e. cutting dermis only) does not improve retrobulbar compartment syndrome. It is the cantholysis that increases the size of the orbital compartment, which is equivalent to a performing a fasciotomy. Do not delay treatment with canthotomy and cantholysis by obtaining a CT scan for further proof of haemorrhage.
- Orbital fractures can also result in entrapment of extraocular muscles within the bony fracture site. Repair within 48 hours of onset is recommended to avoid muscle ischaemia and permanent damage; thus, consult an ophthalmic specialist to evaluate for this condition. Larger fractures with significant bony displacement are less likely to cause muscle belly impingement and ischaemia. Larger fractures usually occur in adults; entrapment and smaller fractures are more common in children, whose bones are less brittle.
Chemical burns
- Chemical burns are true ocular emergencies and must be treated as soon as the patient arrives. Chemical burns can seriously and permanently damage the epithelium of the conjunctiva and cornea and cause ischaemia of the conjunctival and scleral vessels.
- Initial treatment involves copious irrigation of the affected eye and requires little equipment. Ideally, a litre of normal saline or lactated ringers (use tap water only when sterile solutions are not available) is connected to a Morgan lens. Place the lens in the eye, and tilt the patient’s head so that the fluid runs out toward the temple (not into the other eye). If a Morgan lens is not available, cut a length of IV tubing bluntly to maximise flow. When possible, the patient can hold the tip of the tubing on the nasal aspect of the eye so the water runs out of the eye. When both eyes require irrigation, you can connect a nasal cannula to fluid and place it over the bridge of the nose so it drains into both eyes. Be sure to call the ophthalmic specialist at this time to notify them of the situation.
- While flushing the patient’s eye, obtain details about the chemical. For example, is it acid or base, and is it a liquid, powder, or other solid material? Alkaline solutions are usually more damaging to the eye and often require more flushing to normalise the pH (~ 7.0). This is because the saponify phospholipid membranes, leading to rapid epithelial cell death and caustic penetration into the eye. Powders have small granules that can easily get stuck in the superior and inferior fornices of the eye. This situation sometimes requires inverting the eyelids and directly flushing with saline through a 10 mL syringe to dislodge the granules.
- After each litre of solution, or about every 30 minutes, stop the fluid, wait 5 to 10 minutes, and check the pH of the tears. While you are waiting, it is ideal to start the eye exam. Urine dipsticks can be used safely to measure the ocular pH. When the pH is neutral (~ 7.0) you may stop irrigating the eye. If the pH is not neutral, continue this cycle of irrigation, flushes to the fornix, and pH checking until the tears are neutral. This process may require hours of time and liters of saline, so patience and perseverance are crucial.
- If you are in doubt about whether all chemical has been cleared from the eye, continue to flush until the ophthalmologist arrives to examine the patient. Based on the ophthalmic exam, treatment will likely include antibiotic ointments, oral pain medications, and possible drops for inflammation and elevated eye pressure.
- Prognosis after chemical injury depends on:
- The pH concentration of the chemical
- Duration of contact with the ocular surface
- How quickly and adequately the eye is irrigated after chemical injury
Open globe injury
- Open globes include eye injuries that have full-thickness penetration through the sclera or cornea. The size and extent of penetrating injuries varies considerably. Some injuries are so small that a microscope is required for diagnosis; others involve visible foreign bodies still lodged in the eye.
- Signs of an open globe include a peaked pupil, shallow anterior chamber, corneal or scleral laceration, abnormal pigmented tissue pushing through the sclera or cornea, and the presence of many floating red or white blood cells (seen on slit lamp examination) in the aqueous humor fluid.
- A Seidel test can locate small leaks of aqueous fluid from the anterior chamber. To perform a Seidel test, anaesthetise the eye, wet the fluorescein strip, and wipe the strip over the area of concern while keeping the patient from blinking. The undiluted fluorescein appears dark orange in normal light; but if a leak is present, it becomes light orange or green when viewed under blue light.
- Although many ocular trauma scores have been developed to determine the degree and prognosis of globe injury, initial treatment of all open globes is the same. Once the condition is identified, immediately consult an ophthalmic specialist and describe the situation. Prepare the patient for surgery or transfer, because open globes are surgical emergencies that require immediate intervention in haemodynamically stable patients.
- While awaiting patient transfer or specialist consultation, follow this procedure:
- Cover the affected eye with a rigid shield. If a foreign body is sticking out of the eye, cut a foam or paper cup to accommodate the foreign body. Never place a pressure dressing, gauze, or other soft material under the rigid shield because pressure may force contents out of the eye. Furthermore, gauze or soft eye pads can stick to extruding iris or other ocular contents, which might then be pulled out of the eye when removing the pad.
- Provide an IV antibiotic. Fluoroquinolones are the only class of antibiotics that penetrate the vitreous at therapeutic concentrations when given by an intravenous or oral route. IV formulations are preferred for patients with oral restrictions awaiting surgery. If fluoroquinolones are unavailable, give IV broad-spectrum antibiotics to cover both gram-negative and gram-positive bacteria. Be sure the patient is up to date with tetanus immunisation.
- Explain to the patient the importance of minimising eye movement if possible. Extraocular muscle movement can cause further extrusion of intraocular contents. Eye movements are linked in the brain, so moving the good eye causes the injured eye to move as well.
- Treat pain, nausea, and coughing. Valsalva maneuvers can increase pressure on the back of the eye (through the venous system), so reduce these activities to help keep intraocular contents inside of the eye. If the patient is intubated or has an airway in place, ensure that he or she is not getting excessive positive pressure or coughing.
- Minimise manipulation of the eye. Do not perform any examination beyond visual acuity and observation. This is the extent of evaluation necessary before the ophthalmologist arrives.
- Order a CT scan (only if the patient will be treated in your facility) with fine cuts through the orbits to look for a foreign body or other ocular injuries. Each hospital has a slightly different orbital protocol for this, but generally the cuts are 1 mm or less. IV contrast is not required.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |