

Trauma
This was previously featured in an exam

A 13 year old boy is brought to ED by his parents with ankle pain after falling awkwardly on his ankle while skateboarding. He is unable to weight bear. His ankle x-ray is shown. What is the diagnosis?
Answer:
This is an uncommon fracture, unique to adolescents because the distal tibial physis fuses from the medial to the lateral side. Beyond 16 years, the physis is closed and these injuries are not seen. It occurs in the ankle of the young person (between a narrow window of approx. 12-16 years only) when a forced hyper-flexion and/or supination occurs at the ankle. It is characterised by a Salter–Harris type III fracture through the anterolateral aspect of the distal tibial epiphysis with variable amounts of displacement. Caution is required with Tillaux fractures because the Ottawa ankle rules applied to these injuries can miss them. This is because it is not uncommon for the patient to be able to weight bear and the defined bony points are non-tender. The tenderness is usually elicited at the anterior ankle joint line which Ottawa does not describe.Salter-Harris Classification
Trauma
Last Updated: 9th July 2025
Injuries to the traction epiphyses are avulsion injuries. Injuries to the pressure epiphyses at the end of long bones adjacent to the articular surface have been classified into five types— the Salter–Harris classification.
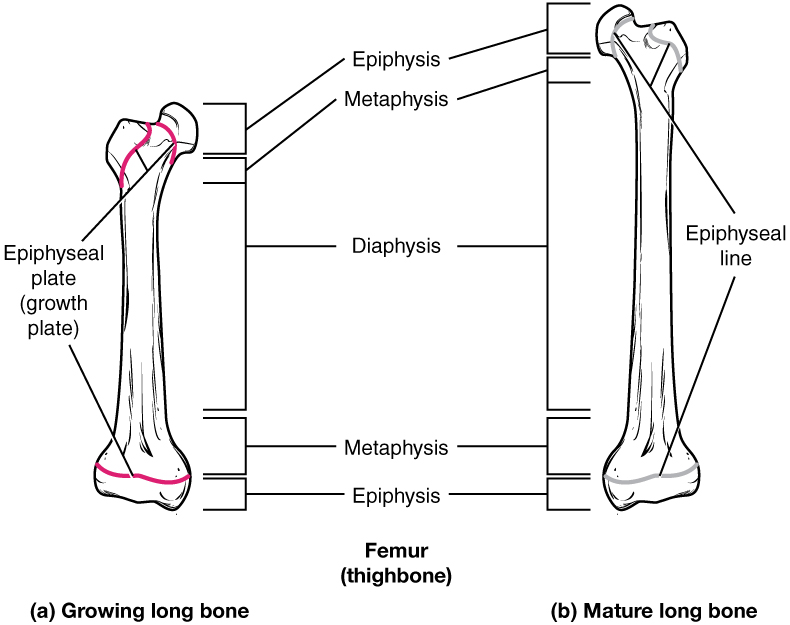
Bone Anatomy in Children. (Image by OpenStax College [CC BY 3.0 , via Wikimedia Commons)
Classification
Note that Salter– Harris types I and V may not be apparent on the initial X- ray.
- Type I (5-7%)
- Fracture plane passes all the way through the growth plate, not involving the bone
- Type II (~75%)
- Fracture plane passes across most of the growth plate and up through the metaphysis
- Type III (7-10%)
- Fracture plane passes some distance along the growth plate and down through the epiphysis
- Type IV (10%)
- Fracture plane passes directly through the metaphysis, growth plate and down through the epiphysis
- Type V (<1%)
- Crushing type injury does not displace the growth plate but damages it by direct compression
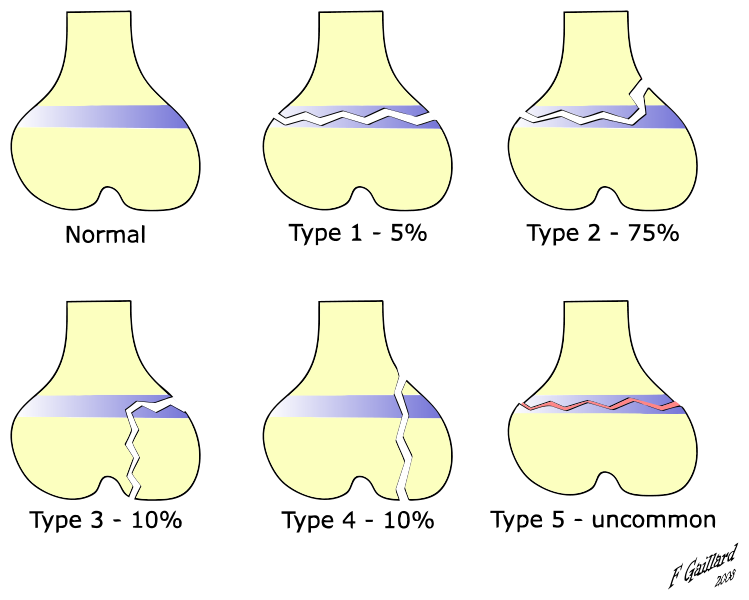
Salter-Harris Classification. (Image by Dr Frank Gaillard (MBBS, FRANZCR) ). The original uploader was Benweatherhead at English Wikipedia derivative work: Zerodamage (This file was derived from) [CC BY-SA 3.0 , via Wikimedia Commons)
- 1 = Slip
- 2 = Above the physis (through metaphysis)
- 3 = Lower than the physis (through epiphysis)
- 4 = Through (metaphysis, growth plate and epiphysis)
- 5 = Ram (a crushing type injury)
Epiphyseal growth plate injury
A concern specific to any epiphyseal injury is that premature fusion of a growth plate may result, with resultant limb shortening and deformity. The risk correlates to some extent with the mechanism of injury and amount of force involved. The different Salter– Harris fractures carry a different level of risk of long- term growth plate problems. The risk is low for types I and II (particularly if undisplaced), moderate for type III, and highest for types IV and V. Problems are usually averted if Salter– Harris type III and IV injuries are accurately reduced and held (e.g. by internal fixation). Type V fractures are notoriously difficult to diagnose and often complicated by premature fusion— fortunately, they are relatively rare.
Tillaux fracture
This is an uncommon fracture, unique to adolescents because the distal tibial physis fuses from the medial to the lateral side. Beyond 16 years, the physis is closed and these injuries are not seen.
It occurs in the ankle of the young person (between a narrow window of approx. 12-16 years only) when a forced hyper-flexion and/or supination occurs at the ankle.
It is characterised by a Salter–Harris type III fracture through the anterolateral aspect of the distal tibial epiphysis with variable amounts of displacement.
Caution is required with Tillaux fractures because the Ottawa ankle rules applied to these injuries can miss them. This is because it is not uncommon for the patient to be able to weight bear and the defined bony points are non-tender. The tenderness is usually elicited at the anterior ankle joint line which Ottawa does not describe.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |