

Respiratory
A 64 year old man presents to the Emergency Department with a 2 hour history of pleuritic chest pain and shortness of breath. He has a past medical history of COPD secondary to occupational exposure and smoking. His observations are recorded as:
- Heart rate: 106 beats per minute
- Blood pressure: 143/87 mmHg
- Respiratory rate: 24 breaths per minute
- Oxygen saturations: 92% on air
- Temperature: 37.3°C
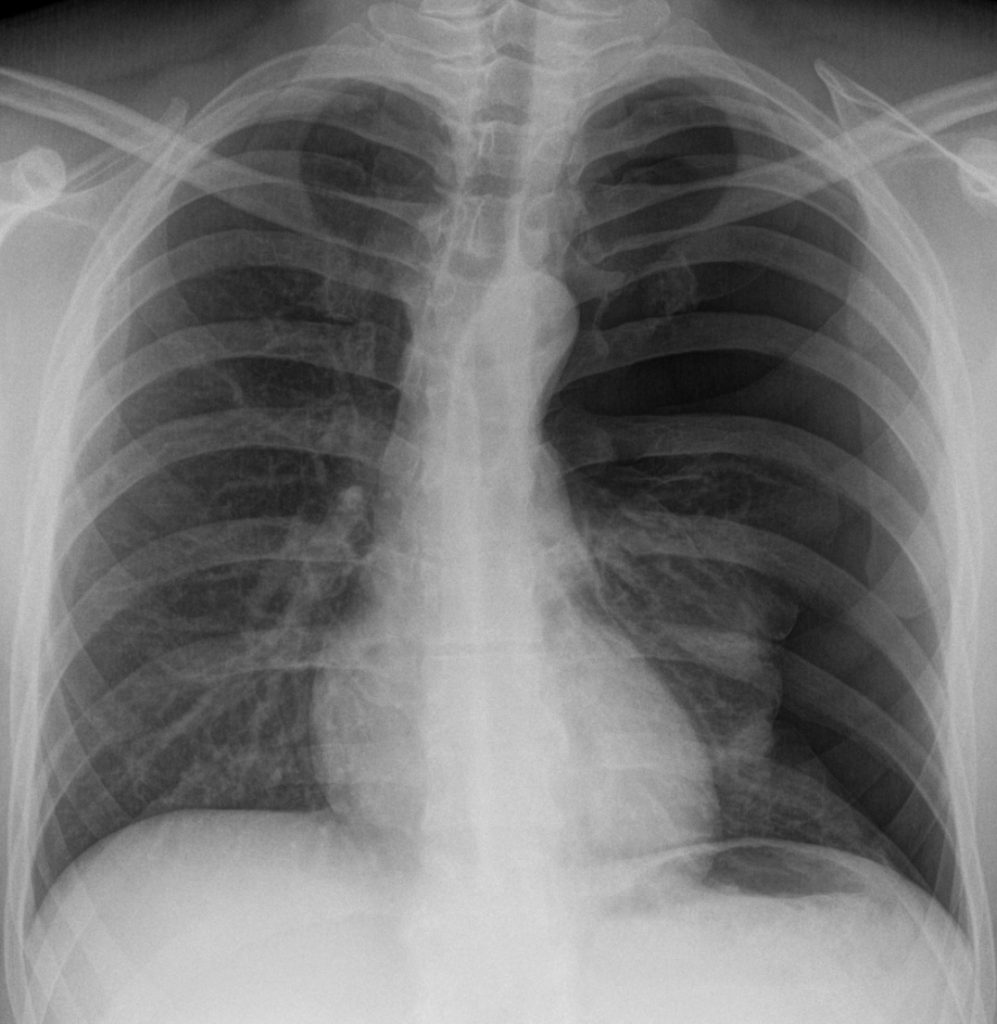
A chest x-ray is performed. How should this patient be managed?
Answer:
The x-ray shows a large left sided pneumothorax. The patient is symptomatic with high risk characteristics (underlying lung disease and > 50 years of age with significant smoking history). The pneumothorax is of sufficient size making it safe to intervene therefore management is with chest drain insertion with regular inpatient review.Spontaneous Pneumothorax
Respiratory
Last Updated: 7th November 2023
The term pneumothorax describes air in the pleural space and is characterised as spontaneous in the absence of trauma or causative medical intervention.
Definitions
- Primary spontaneous pneumothorax (PSP)
- Occurs in patients in the absence of suspected lung disease.
- This distinction does not imply that patients with PSP have normal underlying lung parenchyma, with the majority demonstrating emphysema-like pulmonary changes on CT imaging, but instead reflects that current management and outcomes differ between the two patient groups.
- Secondary spontaneous pneumothorax (SSP)
- Occurs in patients with established underlying lung disease.
- Spontaneous pneumothorax should also be treated as secondary in patients > 50 years of age with a smoking history .
- SSP is most commonly associated with COPD, but may also be associated with TB, asthma, pneumonia, sarcoidosis, cystic fibrosis, malignancy, bronchiectasis, pulmonary fibrosis and AIDs.
Risk factors
Risk factors for primary spontaneous pneumothorax:
- Tall, thin males
- Marfan’s syndrome
- Ehlers-Danlos syndrome
- Alpha-1 antitrypsin deficiency
- Smoking
Clinical features
- Symptoms
- Dyspnoea
- Tachypnoea
- Chest pain
- Signs
- Reduced expansion on affected side
- Reduced air entry on affected side
- Hyperresonance on affected side
- Reduced vocal/tactile fremitus on affected side
In PSP, the symptoms do not correlate closely with the size of the pneumothorax. In many cases the symptoms are mild and approximately half of patients will present after more than 2 days of symptoms. In SSP, symptoms are often more severe than those associated with a primary pneumothorax because lung function may already have been compromised by the underlying pathological process.When severe symptoms are accompanied by signs of cardiorespiratory distress, tension pneumothorax must be considered.
Investigations
- Standard erect PA chest x-ray in inspiration
- Visible visceral pleural edge seen as a very thin, sharp white line
- Absent chest markings peripheral to this line
- Peripheral space is radiolucent compared to adjacent lung
- Small pleural effusions are sometimes seen
- CT scanning for complex or uncertain cases
- This can be regarded as the ‘gold standard’ in the detection of small pneumothoraces and in size estimation. It is also useful in the presence of surgical emphysema and bullous lung disease and for identifying aberrant chest drain placement or additional lung pathology.
- Arterial blood gas (ABG)
- Arterial blood gas measurements are frequently abnormal in patients with pneumothorax, with the arterial oxygen tension (PaO2) being <10.9 kPa in 75% of patients but analysis is not required if oxygen saturations are adequate (> 92%) on breathing room air.
Management
New BTS clinical pathway (July 2023):
- Is the patient symptomatic?
- If no:
- Conservative care
- PSP: regular review as outpatient (every 2-4 days)
- SSP: inpatient review
- If stable, follow up in OPD in 2-4 weeks
- If yes:
- Assess for high risk characteristics
- Haemodynamic compromise (tension pneumothorax)
- Significant hypoxia
- Bilateral pneumothorax
- Underlying lung disease
- > 50 years of age with significant smoking history
- Haemopneumothorax
- Assess for high risk characteristics
- If no:
- Does the patient have high risk characteristics?
- If yes, and it's not safe to intervene (pneumothorax of sufficient size):
- CT imaging and reassess
- If yes, and it's safe to intervene (pneumothorax of sufficient size):
- Chest drain
- Regular inpatient review
- Remove drain when resolved
- Talc pleurodesis can be considered on the first episode of pneumothorax in high risk patients in whom pneumothorax would be hazardous (e.g. severe COPD)
- Discharge and review in OPD in 2-4 weeks
- If no, and it's not safe to intervene (pneumothorax of sufficient size):
- Conservative care as for asymptomatic patient above
- If no, and it's safe to intervene, consider (take into account patient preference and local availability):
- Conservative care as for asymptomatic patient above
- Ambulatory device
- Regular review as outpatient (every 2-3 days)
- Remove device when resolved
- Needle aspiration
- If resolved (improved symptoms and sustained improvement on CXR), discharge and review in OPD in 2-4 weeks
- If not resolved, chest drain
- If yes, and it's not safe to intervene (pneumothorax of sufficient size):
N.B. Pneumothorax of sufficient size to intervene depends on clinical context but, in general, usually ≥ 2 cm laterally or apically on CXR, or any size on CT scan which can be safely accessed with radiological support
Discharge and follow-up
- Patients should be advised to return to hospital if increasing breathlessness develops
- All patients should be followed up by respiratory specialists until full resolution
- Air travel should be avoided for at least a week after chest x-ray has confirmed full resolution
- Diving should be avoided permanently (unless the patient has undergone bilateral surgical pleurectomy and has normal lung function and chest CT scan postoperatively)
- All patients should be advised to stop smoking (reduces risk of recurrence)
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |