

Respiratory
This was previously featured in an exam
A 41 year old lady, with a previous history of DVT, presents to the Emergency Department with sudden onset dizziness, right sided pleuritic chest pain, and shortness of breath. She has no other past medical history, and is not currently taking any regular medication. She returned to the UK from a trip to Australia 3 days ago. Her observations are recorded as:
- Heart rate: 110 beats per minute
- Blood pressure: 110/70 mmHg
- Respiratory rate: 26 breaths per minute
- Oxygen saturations: 92% on air
- Temperature: 37.6°C
You suspect pulmonary embolism. What is this patient's Wells score?
Answer:
If PE is suspected, use the two-level PE Wells score to estimate the clinical probability of PE:- Clinical signs and symptoms of DVT (3 points)
- An alternative diagnosis is less likely than PE (3 points)
- Heart rate > 100 bpm (1.5 points)
- Immobilisation for at least 3 days, or surgery in the previous 4 weeks (1.5 points)
- Previous objectively diagnosed PE or DVT (1.5 points)
- Haemoptysis (1 point)
- Malignancy - receiving treatment, treated in the last 6 months, or palliative (1 point)
Pulmonary Embolism
Respiratory
Last Updated: 21st April 2023
Definitions
- Pulmonary embolism (PE) is a condition in which one or more emboli, usually arising from a thrombus formed in the veins (or, rarely, in the right heart), are lodged in and obstruct the pulmonary arterial system, causing severe respiratory dysfunction.
- Provoked PE is associated with an antecedent (within 3 months) and transient risk factor, such as significant immobility, surgery, trauma, pregnancy or puerperium, and the use of the combined contraceptive pill or hormone replacement therapy. These risk factors can be removed, thereby reducing the risk of recurrence.
- Unprovoked PE occurs in the absence of a transient risk factor. The person may have no identifiable risk factor or a risk factor that is persistent and not easily correctable (such as active cancer or thrombophilia). Because these risk factors cannot be removed, the person is at an increased risk of recurrence.
Pathophysiology
In pulmonary embolism, lung tissue is ventilated but not perfused, producing an intra-pulmonary dead space and resulting in impaired gas exchange.
The area of lung that is no longer perfused by the pulmonary artery may infarct, but often does not do so because oxygen continues to be supplied by the bronchial circulation and the airways. This leads to a reduction in the cross-sectional area of the pulmonary arterial bed, which results in an elevation of pulmonary arterial pressure and a reduction in cardiac output. After several hours, alveolar collapse occurs, which worsens hypoxaemia. Large or multiple emboli can abruptly increase pulmonary arterial pressure to a level of afterload that cannot be matched by the right ventricle. Sudden death may occur, or the person may present with hypotension or syncope, which might progress to shock or death due to acute right ventricular failure.
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare complication of PE. In people with CTEPH, emboli are replaced over months or years by fibrous tissue, leading to chronic obstruction of the pulmonary arterial vasculature, progressive increases in pulmonary arterial pressure, and, if untreated, right heart failure. Inadequate anticoagulation, large thrombus mass, residual thrombi, and recurrence of VTE may contribute to the development of CTEPH.
Sources of emboli:
- Deep vein thrombosis
- Tumours (most commonly prostate and breast)
- Fat (from long-bone fractures)
- Amniotic fluid in pregnant women
- Foreign bodies (e.g. during intravenous drug use)
- Air (e.g. admitted during surgery)
- Sepsis (e.g. infective endocarditis)
Risk factors
About 30–50% of venous thromboembolism (VTE) episodes do not have an identifiable risk factor. The remaining episodes are caused by transient or persistent factors that increase the risk of VTE by inducing hypercoagulability, venous stasis, or vascular wall damage or dysfunction (known collectively as Virchow’s triad).
- Major risk factors
- Current DVT
- Previous DVT/PE
- Active malignancy
- Recent surgery, hospitalisation, lower limb trauma or other immobilisation
- Pregnancy and up to 6 weeks postpartum
- Other risk factors
- Increasing age (> 60 years)
- Combined oral contraceptive pill and HRT
- Obesity (BMI > 30 kg/m2)
- Long-distance sedentary travel
- Varicose veins
- Superficial venous thrombosis
- Thrombophilias
- Medical comorbidities
Clinical features
- Symptoms
- Dyspnoea
- Tachypnoea
- Pleuritic chest pain
- Cough and haemoptysis
- Dizziness and/or syncope
- Symptoms of DVT
- Signs
- Tachycardia
- Hypotension
- Hypoxaemia
- Pyrexia
- Elevated jugular venous pressure
- Gallop rhythm, a widely split second heart sound, tricuspid regurgitant murmur
- Pleural rub
- Signs of DVT
Investigations
- ECG
- An ECG should be obtained to look for signs supportive of right heart strain such as right axis deviation, and to rule out an acute coronary syndrome
- ECG signs that may be present include: sinus tachycardia, non-specific ST-segment and T-wave abnormalities, right axis deviation, incomplete or complete right bundle-branch block, and, less commonly, T-wave inversion in leads V1–V3, P pulmonale (peaked P wave in lead II), or the classical S1, Q3, T3 (deep S wave in lead 1, Q wave in lead 3, and T-wave inversion in lead 3)
- Chest x-ray
- The main purpose of the chest radiograph is to exclude conditions and look for alternative diagnosis such as pneumothorax or infection which may give rise to the same presenting symptoms
- Chest x-ray features that may be present include: atelectasis, pleural effusion, or elevation of a hemidiaphragm
- Arterial blood gas if indicated by oxygen saturations (< 92%)
- ABG analysis may confirm hypoxia, evidence of hyperventilation and an increased arterial-alveolar gradient
- D-dimer testing if indicated by Wells score
- Computed tomographic pulmonary angiography (CTPA)
- The investigation of choice for most people with high clinical probability of PE, or non-high clinical probability and a positive D-dimer test.
- V/Q (ventilation-perfusion) scan
- May be carried out in some circumstances e.g. pregnancy, or in patients with normal CXR and no chronic cardiac/respiratory disease
- Lower limb compression venous ultrasound
- May be useful for pregnant women in whom irradiation from other imaging may be harmful
- Echocardiography
- For people with hypotension (clinically 'massive' PE). The absence of right heart failure excludes PE.
- Signs of right heart strain on echocardiography include:
- Dilation of the right ventricle (RV) and hypokinesis of the free wall is the most common sign of RV strain. McConnell's sign is a distinct echocardiographic feature of acute massive pulmonary embolism, defined as right ventricular free wall akinesis with sparing of the apex. As a simple guide, the right ventricle is normally 60% of the size of the left ventricle. If the right ventricular diameter is approaching or greater than that of the left ventricle, there is significant enlargement.
- Paradoxical septal motion, expressed as bowing of the interventricular septum into the LV outflow tract. This is best observed in the parasternal short view, but can also be seen in the long axis.
- Inferior vena cava (IVC) distension or non-collapsibility may be noted.
- Occasionally, the severity of RV dilation can lead to valvular dysfunction, usually tricuspid regurgitation.
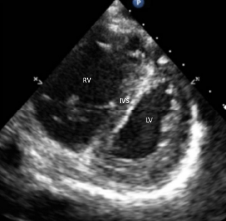
Bowing of the interventricular septum (IVS) into left ventricle is visualised as “D-sign” on a parasternal short-axis view in a patient with right ventricular (RV) failure.
PE Wells Score
If PE is suspected, use the two-level PE Wells score to estimate the clinical probability of PE:
- Clinical signs and symptoms of DVT (3 points)
- An alternative diagnosis is less likely than PE (3 points)
- Heart rate > 100 bpm (1.5 points)
- Immobilisation for at least 3 days, or surgery in the previous 4 weeks (1.5 points)
- Previous objectively diagnosed PE or DVT (1.5 points)
- Haemoptysis (1 point)
- Malignancy - receiving treatment, treated in the last 6 months, or palliative (1 point)
Wells score ≤ 4 points – PE unlikely:
- Offer a D-dimer test with the result available within 4 hours if possible.
- If the D-dimer test result cannot be obtained within 4 hours, offer interim therapeutic anticoagulation while awaiting the result.
- If the D-dimer test result is positive: follow the actions below as for Wells score > 4 points.
- If the D-dimer test result is negative: stop interim therapeutic anticoagulation and consider an alternative diagnosis.
Wells score > 4 points – PE likely:
- Offer a computed tomography pulmonary angiogram (CTPA) immediately if possible OR
- For people with an allergy to contrast media, severe renal impairment (estimated creatinine clearance less than 30 ml/min) or a high risk from irradiation, assess the suitability of a ventilation/perfusion single photon emission computed tomography (V/ Q SPECT) scan or, if a V/Q SPECT scan is not available, a V/Q planar scan, as an alternative to CTPA.
- If a CTPA, V/Q SPECT or V/Q planar scan cannot be done immediately, offer interim therapeutic anticoagulation.
- If PE is identified by CTPA, V/Q SPECT or V/Q planar scan:
- Offer or continue anticoagulation treatment OR
- If anticoagulation treatment is contraindicated, consider a mechanical intervention OR
- For people with PE and haemodynamic instability, consider thrombolytic therapy
- If PE is not identified by CTPA, V/Q SPECT or V/Q planar scan:
- Consider a proximal leg vein ultrasound scan if DVT is suspected
- If DVT is not suspected: stop interim therapeutic anticoagulation and consider an alternative diagnosis
Management
- Anticoagulation
- Carry out baseline blood tests including full blood count, renal and hepatic function, prothrombin time (PT) and activated partial thromboplastin time (APTT) before starting anticoagulation (but do not wait for the results before starting treatment)
- When using interim therapeutic anticoagulation for suspected PE, if possible, choose an interim anticoagulant that can be continued if PE is confirmed
- Offer either apixaban or rivaroxaban to people first line unless contraindicated
- If neither apixaban nor rivaroxaban is suitable offer:
- LMWH for at least 5 days followed by dabigatran or edoxaban or
- LMWH concurrently with a vitamin K antagonist (VKA) for at least 5 days, or until the INR is at least 2.0 in 2 consecutive readings, followed by a VKA on its own
- Do not routinely offer unfractionated heparin (UFH) with a VKA to treat confirmed PE unless the person has renal impairment or established renal failure or an increased risk of bleeding
- Offer anticoagulation treatment for at least 3 months to people with confirmed PE
- Thrombolytic therapy
- Thrombolytic therapy may be used to remove the embolic material from the pulmonary arteries by promoting lysis of blood clots
- Consider pharmacological systemic thrombolytic therapy for people with PE and haemodynamic instability
- Do not offer pharmacological systemic thrombolytic therapy to people with PE and haemodynamic stability with or without right ventricular dysfunction
- Mechanical interventions
- Inferior vena cava (IVC) filters are designed to trap fragmented thromboemboli from the deep leg veins en route to the pulmonary circulation (whilst preserving blood flow in the IVC filter)
- Various filters are available and can be placed in the IVC filter on either a temporary basis (for example in people with PE who cannot have anticoagulation treatment) or a permanent basis (for example in people with recurrent PE despite adequate anticoagulation treatment after alternative treatments have been considered)
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |