

Cardiology
This was previously featured in an exam
This was previously featured in an exam
Question 46 of 180
A 34 year old man presents to ED with palpitations and dizziness. ECG shows a broad-complex tachycardia. Which of the following features is more suggestive of supraventricular tachycardia (SVT) with aberrancy rather than ventricular tachycardia?
Answer:
Regular broad complex tachycardias can be ventricular (VT) or supraventricular (SVT with aberrancy) in origin. Unfortunately, the electrocardiographic differentiation of VT from SVT with aberrancy is very difficult. Electrocardiographic features that increase the likelihood of VT include:- Absence of typical RBBB or LBBB morphology
- Extreme axis deviation (“northwest axis”): QRS positive in aVR and negative in I and aVF
- Very broad complexes > 160ms
- AV dissociation: P and QRS complexes at different rates (P waves are often superimposed on QRS complexes and may be difficult to discern)
- Capture beats: Occur when the sinoatrial node transiently “captures” the ventricles in the midst of AV dissociation, producing a QRS complex of normal duration
- Fusion beats: Occur when a sinus and ventricular beat coincide to produce a hybrid complex
- Positive or negative concordance throughout the precordial leads (no rS complexes seen)
- RSR’ complexes with a taller left rabbit ear (in contrast to RBBB, where the right rabbit ear is taller)
- Brugada sign: Distance from onset of R wave to nadir of S wave is > 100ms in leads V1-6
- Josephson sign: Notching/slurring near the nadir of the S wave
Heart Block and Conduction Abnormalities
Cardiology
Last Updated: 16th May 2023
Atrioventricular (AV) heart block
- First degree AV block
- Prolongation of PR interval (>0.2s)
- Second degree AV block Mobitz type I
- Progressive prolongation of PR interval after each successive P wave with eventual dropped ventricular conduction
- Second degree AV block Mobitz type II
- Constant (often prolonged) PR interval with random intermittent dropping of ventricular conduction
- Second degree AV block (2:1 type) block
- Alternate P waves not conducted to ventricles; alternate P waves not followed by QRS complex
- Third degree (complete) AV block
- Complete dissociation between atria and ventricles; no relationship between P waves and QRS complex
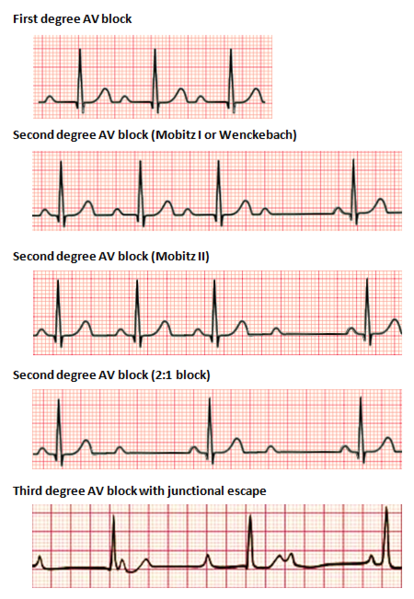
Types of Heart Block. (Image by Npatchett, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons)
Bundle Block
- Left anterior fascicular block (LAFB)
- Left axis deviation (leads I/avL are positive, leads II/III/avF are negative)
- qR complexes in I, aVL (small Q waves and tall R waves)
- rS complexes in II, III, aVF (small R waves and deep S waves)
- No evidence of LVH
- Left posterior fascicular block (LPFB)
- Right axis deviation (leads I/avL are negative, leads II/III/avF are positive)
- rS complexes in I, aVL (small R waves and deep S waves)
- qR complexes in II, III, aVF (small Q waves and tall R waves)
- No evidence of RVH
- Left bundle branch block (LBBB)
- QRS duration > 120 ms
- Dominant S wave in V1
- Broad monophasic R wave in lateral leads (I, aVL, V5-6)
- Absence of Q waves in lateral leads
- Prolonged R wave peak time > 60ms in leads V5-6
- Right bundle branch block (RBBB)
- QRS duration > 120 ms
- RSR pattern in in V1-V3 (M-shaped QR complex)
- Wide, slurred S wave in lateral leads (I, aVL, V5-6)
- Bifascicular block presents with one of two ECG patterns:
- RBBB + LAFB manifests as left axis deviation
- RBBB + LPFB manifests as right axis deviation
- Trifascicular block
- True trifascicular block presents with one of two ECG patterns:
- 3rd degree AV block + RBBB + LAFB
- 3rd degree AV block + RBBB + LPFB
- Clinically, trifascicular block is most commonly used to describe:
- bifascicular block + 1st degree AV block or 2nd degree AV block
- True trifascicular block presents with one of two ECG patterns:
*LAD = left axis deviation, RAD = right axis deviation
VT vs SVT with aberrancy
Differentiating between SVT with aberrancy versus VT can be very difficult.
Clinical factors associated with VT or SVT:
- The likelihood of VT is increased with:
- Age > 35 (positive predictive value of 85%)
- Structural heart disease
- Ischaemic heart disease
- Previous MI
- Family history of sudden cardiac death (suggesting conditions such as HOCM, congenital long QT syndrome, Brugada syndrome or arrhythmogenic right ventricular dysplasia that are associated with episodes of VT)
- The likelihood of SVT with aberrancy is increased if:
- Previous ECGs show a bundle branch block pattern with identical morphology to the broad complex tachycardia
- Previous ECGs show evidence of WPW (short PR < 120ms, broad QRS, delta wave)
- The patient has a history of paroxysmal tachycardias that have been successfully terminated with adenosine or vagal manoeuvres
ECG features associated with VT or SVT:
- Electrocardiographic features that increase the likelihood of VT include:
- Absence of typical RBBB or LBBB morphology
- Extreme axis deviation (“northwest axis”): QRS positive in aVR and negative in I and aVF
- Very broad complexes > 160ms
- AV dissociation: P and QRS complexes at different rates (P waves are often superimposed on QRS complexes and may be difficult to discern)
- Capture beats: Occur when the sinoatrial node transiently “captures” the ventricles in the midst of AV dissociation, producing a QRS complex of normal duration
- Fusion beats: Occur when a sinus and ventricular beat coincide to produce a hybrid complex
- Positive or negative concordance throughout the precordial leads (no rS complexes seen)
- RSR’ complexes with a taller left rabbit ear (in contrast to RBBB, where the right rabbit ear is taller)
- Brugada sign: Distance from onset of R wave to nadir of S wave is > 100ms in leads V1-6
- Josephson sign: Notching/slurring near the nadir of the S wave
Brugada criteria for ventricular tachycardia:
- Is there an absence of an RS complex in all precordial leads?
- If yes = VT
- If no = next question
- Is the R to S interval >100 msec (2.5 small boxes) in one precordial lead?
- If yes = VT
- If no = next question
- Is there atrioventricular (AV) dissociation?
- If yes = VT
- If no = next question
- Is there morphology criteria for VT present in precordial leads V1/V2 and V6?
- If yes = VT
- If no = SVT with aberrancy
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |