

Trauma
This was previously featured in an exam
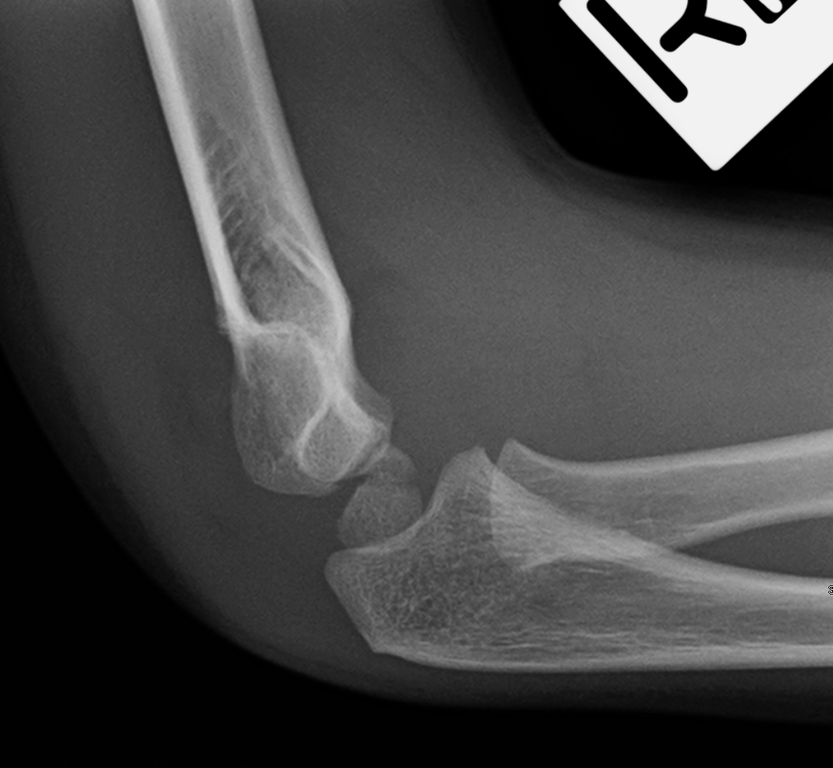
A 4 year old child is brought to the Emergency Department after complaining of pain in the right elbow following a fall from a swing. An x-ray is performed. What is the diagnosis?
Answer:
There is a fat pad sign and the anterior humeral line does not pass through the capitulum. Supracondylar fracture:- These are most common in children but also occur in adults. This typically follows a fall on an outstretched hand.
- The elbow may be grossly swollen and deformed, but the normal triangular relationship of the olecranon and epicondyles is characteristically preserved. Check distal pulses and sensation carefully, as the brachial artery, ulnar, median, and radial nerves can all be damaged.
- 25% of supracondylar fractures are undisplaced and may not be obvious on X- ray, although a joint effusion will be seen (fat pad sign). Most fractures are displaced, angulated, or rotated. The extent of angulation (both in sagittal and coronal planes) is easy to underestimate. Viewed from laterally, the capitulum normally makes an angle of 45° with the humeral shaft. The anterior humeral line (drawn along the front of the humeral shaft on the lateral view) normally passes through the middle of the ossification centre of the capitulum in the distal humerus. Also, the normal carrying angle (seen in AP view) is 10°.
Elbow and Arm Injuries
Trauma
Last Updated: 16th July 2025
General approach
In any injured elbow, look specifically for:
- Elbow effusion (felt as a tense, bulging swelling halfway between the lateral epicondyle and the point of the olecranon).
- The normal relationship between the olecranon and the lateral and medial epicondyles— all should form an equilateral triangle with the elbow flexed.
- Range of movement— X- ray patients who cannot fully extend the elbow and flex to touch the shoulder tip.
The presence of an effusion on X-ray implies that a radial head/ neck or supracondylar fracture is present, even if none is visible. The fat pad sign, also known as the sail sign, is caused by displacement of the fat pad around the elbow joint, and may suggest occult elbow fracture. In children, the most common occult elbow fracture is a supracondylar fracture. In adults, the most common occult fracture of the elbow is a radial head fracture.
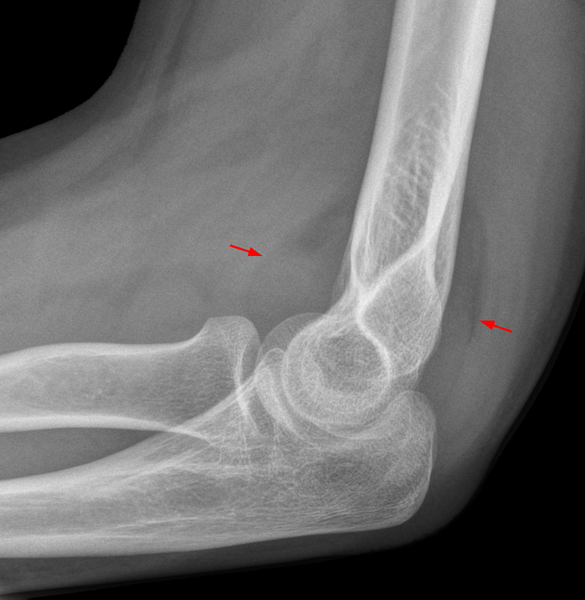
Anterior and posterior fat pad sign in an occult fracture of the radial head. (Image by Hellerhoff / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0))
Elbow ossification
Elbow ossification in children occurs at the six elbow ossification centers in a reproducible order. Being familiar with the order of ossification of the elbow is important in not mistaking an epicondylar fracture for a normal ossification center.
Appearance of elbow ossification centres (CRITOE):
- Capitellum: 1 year
- Radial head: 3 years
- Internal (medial) epicondyle: 5 years
- Trochlea: 7 years
- Olecranon: 9 years
- External (lateral) epicondyle: 11 years
Easy guide: 1-3-5-7-9-11
The order of "I" and "T" are most important to remember; the trochlea ossification center should not appear before the internal (medial) epicondyle ossification centre. If you can see a trochlea but no internal epicondyle, then you need to look very hard for the avulsed internal epicondyle ossification center.
Radial head/neck fracture
- Follow falls onto an outstretched hand (the radial head impacts against the capitellum) or direct trauma to the elbow. It can sometimes occur in combination with a wrist fracture (a dramatic example is the Essex– Lopresti fracture– dislocation.
- Examine movements— extension and flexion are usually limited, but supination and pronation may be relatively normal. Check for an elbow effusion, and palpate for tenderness over the radial head whilst supinating/pronating the elbow.
- X- ray usually confirms elbow effusion, but fractures may be difficult to see.
- Treat fractures with analgesia and a collar and cuff sling. Discharge undisplaced fractures with written advice about exercises and likely recovery time, with advice to return if there are any problems. Arrange a fracture clinic review for displaced or comminuted fractures which may require surgery. If very painful, immobilise in an above- elbow POP backslab at 90°.
Olecranon fracture
- Follow falls onto the point of the elbow. The olecranon fragment may displace proximally due to pull of the triceps.
- Swelling, tenderness, or crepitus are present on examination.
- In the young, the olecranon epiphysis may cause confusion on X- rays.
- Treat undisplaced or hairline fractures in an above- elbow backslab POP at 90°; provide analgesia, and arrange fracture clinic follow- up. Refer fractures that are displaced or involve the elbow joint for ORIF.
Dislocated elbow
- Examination reveals loss of the normal triangular relationship between the olecranon and epicondyles. Check distal pulses and sensation as the brachial artery and the median and ulnar nerves may be damaged.
- Elbow dislocations may be classified according to the direction of dislocation and the presence of associated fractures (e.g. fractured coronoid). The most frequent injury is posterolateral dislocation (i.e. movement of the distal part in a posterolateral direction).
- After analgesia and X- ray, most dislocations may be reduced in the ED under IV sedation with full monitoring. However, GA is sometimes required.
- Reduction techniques for postero-lateral dislocations:
- Flex the elbow to 60° with countertraction on the upper arm. Pull on the fully pronated forearm at this angle. Slight flexion at the elbow may be necessary.
- Alternatively, lever the olecranon forward with both thumbs, whilst holding the elbow flexed and whilst an assistant provides traction on the forearm.
- Reduction is usually confirmed by a ‘clunk’ and restoration of the normal triangular relationship of the elbow landmarks. Once reduced, recheck pulses and sensation; immobilise in an above- elbow POP backslab at 90°, and X- ray again (looking for associated fractures). Consider admission for analgesia and observation for possible significant limb swelling. If unable to reduce, refer for reduction under GA.
Supracondylar fracture
- These are most common in children but also occur in adults. This typically follows a fall on an outstretched hand.
- The elbow may be grossly swollen and deformed, but the normal triangular relationship of the olecranon and epicondyles is characteristically preserved. Check distal pulses and sensation carefully, as the brachial artery, ulnar, median, and radial nerves can all be damaged.
- 25% of supracondylar fractures are undisplaced and may not be obvious on X- ray, although a joint effusion will be seen (fat pad sign). Most fractures are displaced, angulated, or rotated. The extent of angulation (both in sagittal and coronal planes) is easy to underestimate. Viewed from laterally, the capitulum normally makes an angle of 45° with the humeral shaft. The anterior humeral line (drawn along the front of the humeral shaft on the lateral view) normally passes through the middle of the ossification centre of the capitulum in the distal humerus. Also, the normal carrying angle (seen in AP view) is 10°.
- Management in adults: Immobilise in an above-elbow backslab POP, and give analgesia. Refer to the orthopaedic surgeon, as MUA/ ORIF are usually required.
- Management in children: Provide analgesia (eg nasal diamorphine), and refer for manipulation under GA if: neurovascular deficit, >50% displacement, >20° angulation of the distal part posteriorly, >10° medial or lateral angulation. If there is no indication for manipulation under GA, refer for admission and observation if there is much swelling. If no significant angulation, displacement, or swelling, discharge with analgesia, a collar and cuff under a body bandage (elbow at 90°, with confirmed radial pulse present), and fracture clinic follow- up. Consider using a padded backslab POP if significant pain is present.
- Complications include malunion with persistent deformity, nerve damage (particularly radial and median nerve), compartment syndrome, stiffness (including myositis ossificans), neurovascular deficit (e.g. Volkmann’s contracture).
- Fractures of the capitellum occasionally occur in isolation. If undisplaced, treat conservatively with analgesia and POP. Refer those with displaced fractures for specialist treatment (possibly ORIF).
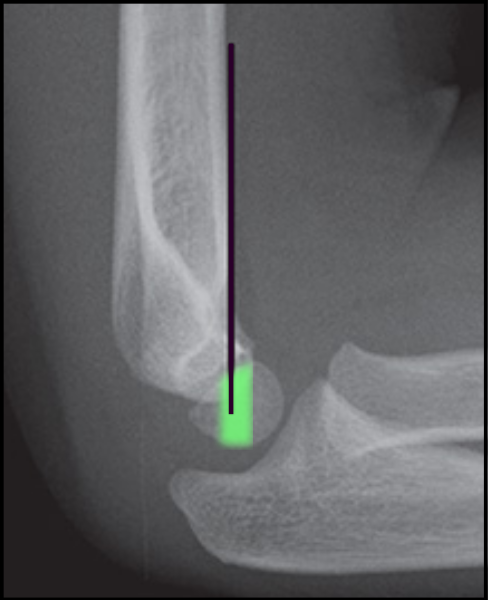
Anterior Humeral Line in a Normal Elbow. (Image by Tracy Kilborn, Halvani Moodley and Stewart Mears, Mikael Häggström / CC BY-SA (https://creativecommons.org/licenses/by-sa/4.0))

Anterior Humeral Line in a Supracondylar Fracture. (Image by James Heilman, MD (Own work) [CC BY-SA 4.0 , via Wikimedia Commons)
Shaft of humerus fracture
- This results from a fall onto an outstretched hand or onto the elbow, or occasionally from excessive twisting (e.g. arm wrestling).
- The fracture may be obvious and palpable. Check distal pulses, sensation, and the elbow joint. Check particularly for injury to the radial nerve which runs close to the humeral shaft in the spiral groove.
- X- ray reveals a transverse, comminuted, or spiral humeral shaft fracture.
- Provide analgesia and support the fracture (e.g. in a POP U- slab from the axilla down to and around the olecranon and up the outside of the upper arm— apply with the elbow flexed to 90°, and hold in place with a bandage). Alternative treatment includes a ‘hanging cast’ POP (above-elbow POP at 90°— the weight of POP and the arm holds the fracture in a satisfactory position).
- Refer if displaced, comminuted, or angulated or if neurovascular complications are suspected. MUA and internal fixation are required in these cases.
- Remember to consider the possibility of NAI in children, especially if the patient is <3y old or the fracture is spiral.
Pulled elbow (traumatic subluxation of the radial head)
- A direct pull on the arm of a child aged 1– 5 years may result in the radial head being pulled out of the annular ligament (‘nursemaid’s elbow’). With sudden pulling on the distal radius, a portion of the annular ligament slips over the head of the radius and slides into the radiohumeral joint where it becomes trapped.
- The child refuses to use the arm. If there is a characteristic history, there is no need to X- ray.
- The traditional reduction technique involves flexing the elbow to 90°, then supinating the elbow fully. However, manipulating the elbow into full pronation may give a better reduction rate. A click is sometimes felt or heard during reduction. If full pronation fails, try full supination and leave for 10 min. Allow the child to play and watch— he will usually use the arm again soon. If he does not, obtain X- rays and senior help. Repeat manipulation can be done once, but if that does not lead to a rapid improvement in function, then place the arm in a sling; give analgesia, and arrange review in 1– 2 days. The elbow may reduce spontaneously or may need further manipulation. Rarely, repeated manipulation is unsuccessful until sedation is given.
- After successful manipulation, advise the parents to avoid pulling the arm forcefully. A pulled elbow may recur up to about age 5 years if the arm is pulled, but after that the child should have no long- term problems with the elbow.
Other elbow injuries in children
- Lateral epicondylar epiphyseal injury
- Salter– Harris type II injury may follow a fall on an outstretched hand. The elbow is swollen, with decreased movement and maximum tenderness on the lateral aspect. X- rays demonstrate the fracture, which may be displaced by the pull of the forearm extensors, requiring surgical reduction. Treat undisplaced fractures with a long arm backslab POP, collar and cuff at 90°, analgesia, and fracture clinic follow- up.
- Medial epicondylar epiphyseal injury
- Maximal tenderness is apparent on the medial side of the elbow. Check carefully for ulnar nerve damage. Refer immediately if the ulnar nerve is involved or if the fracture is displaced. Treat undisplaced fractures with analgesia, collar and cuff at 90° under clothes (confirm the radial pulse is present), and fracture clinic follow- up.
- Radial head/ neck fracture
- The radiocapitellar line is drawn down the axis of the proximal radius on the lateral view of the elbow and should bisect the capitellum. Failure to do so suggests an occult radial neck fracture or radial head dislocation. Most of these fractures can be managed satisfactorily with analgesia, collar and cuff, advice leaflet, and no need for follow- up. Refer to the fracture clinic if there is significant angulation.
- Elbow injury without obvious fracture
- Treat elbow injuries where there is clinical suspicion of fracture, but none seen on X- ray, along the same lines as for an undisplaced fracture (analgesia, collar and cuff, advice leaflet, no follow- up). This includes children who have decreased range of movement and whose X- rays show an elbow effusion (‘fat pad sign’).
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |