

Trauma

A 34 year old woman presents to the Emergency Department after falling on a night out with friends. She is unable to weight bear due to pain in her right knee. An x-ray is performed. What is the diagnosis?
Answer:
Tibial plateau fracture:- Falls onto an extended leg can cause compression fractures of the proximal tibia. Valgus stresses crush or fracture the lateral tibial plateau. These injuries are commonly seen in pedestrians injured following impact with car bumpers. Varus injuries result in crushing or fracture of the medial tibial plateau and are usually associated with rupture of the opposite collateral ligaments.
- Examine for tenderness over the medial or lateral margins of the proximal tibia. Look for swelling, haemarthrosis, or ligamentous instability.
- Look carefully on X- rays for breaks in the articular surfaces of the proximal tibia, avulsions from the ligamentous attachments, or loss of height from the medial and lateral tibial plateau, but beware this may be subtle.
Knee Injuries
Trauma
Last Updated: 14th December 2023
Knee assessment
- Carefully elicit the exact mechanism of injury as it provides clues to the diagnosis:
- Valgus or varus stresses can damage the medial and lateral collateral ligaments, respectively.
- Flexed, twisting knee injuries are frequently associated with meniscal injuries.
- The anterior cruciate ligament (isolated or associated with medial collateral and/ or medial meniscal injuries) may tear during forced flexion or hyperextension.
- Posterior cruciate injuries may follow falls or dashboard impact where the tibia is forced backwards violently (often associated with medial or lateral ligament injuries).
- Take a focussed history:
- Rapid- onset tense swelling in a knee is usually an acute haemarthrosis.
- Swelling developing more gradually over several days is more likely to represent a reactive effusion.
- Ask about previous knee problems: swelling, clicking, locking, or giving way (the last two suggest underlying meniscal pathology).
- Document any previous knee surgery or the presence of other joint problems.
- In a hot, swollen, painful, and stiff knee without a history of significant trauma, consider and exclude septic arthritis.
- On examination:
- Ask patient to walk and assess posture and gait
- Look for bruising, redness, swelling, abrasions/wounds, asymmetry, scars, muscle wasting, fixed deformity
- Palpate for warmth, crepitation, joint line tenderness, bony tenderness, the presence of a knee effusion and for tone and bulk of the quadriceps muscle
- Check straight leg raise: the ability to do this against resistance virtually excludes quadriceps and patellar tendon rupture or transverse patellar fractures
- Assess knee movement: gentle encouragement or supporting the limb may be required, but do not use any force
- Assess the cruciate ligaments - anterior and posterior draw test
- Assess the collateral ligaments - valgus and varus stress tests
- Assess for neurovascular damage
Ottawa knee rules
Obtain X- rays if there is suspected fracture or other significant injury. Use the Ottawa knee rules to assist the decision (in those aged between 18 and 55y) as to whether or not to X- ray.
X- rays are only required if any of the following are present:
- There is isolated bony tenderness of the patella.
- There is bony tenderness over the fibula head.
- The patient cannot flex the knee to 90°.
- The patient cannot weight-bear (take at least four steps), both immediately after the injury and at the time of examination.
Adopt a lower threshold for obtaining X- rays in those aged <18 or >55y, patients intoxicated with alcohol, those suffering from bone disease (e.g. RA, documented osteoporosis), and those who re- attend the ED with the same injury (having not been X- rayed initially). In addition, offer an X-ray of the knee if knee swelling occurs following acute trauma.
Patellar fracture
- This may follow a direct blow or fall onto the patella or sudden violent knee flexion or contraction of the quadriceps muscle.
- Look for pain, swelling, crepitus, and difficulty extending the knee. Displaced transverse fractures result in an inability to straight leg raise (this is also a feature of rupture of the quadriceps tendon or patellar tendon). There may be associated haemarthrosis.
- X- rays may be difficult to interpret, as the patella overlies the distal femur on the AP view and can obscure subtle fractures. Take care not to mistake a bipartite patella for a fracture (the accessory bone is typically in the upper, lateral part of the patella).
- Treat vertical fractures with analgesia; immobilise in a non- weightbearing above- knee POP backslab; supply crutches, and arrange orthopaedic follow- up.
- Transverse fractures tend to displace due to the pull of the quadriceps. Treat with analgesia and immobilisation in a POP backslab, and refer to the orthopaedic team for probable ORIF (occasionally, the orthopaedic team may treat an undisplaced transverse fracture conservatively).
Dislocation of the patella
- The patella typically dislocates laterally. This often follows medial stress to the knee— the dislocation may reduce spontaneously. There may be a history of recurrent dislocation.
- The patient has a painful knee, held in flexion, with obvious lateral displacement of the patella.
- X- rays are not generally required prior to reduction of the dislocation.
- Reduction can usually be achieved using Entonox®— IV analgesia is seldom required.
- Stand on the lateral side of the affected limb and hold the affected knee gently. Using a thumb, lever the patella medially in one smooth, firm movement, whilst gently extending the knee at the same time. Successful reduction is obvious and should rapidly relieve symptoms. Once reduced, obtain X-rays, immobilise in a canvas (‘cricket pad’) back- splint or backslab cast POP, provide analgesia, and arrange orthopaedic follow- up.
- An MRI scan at follow- up may help to identify the extent of damage to the medial patellofemoral ligament— a knee specialist will decide about possible surgical repair.
- The patient who has experienced spontaneous reduction and/ or subluxation prior to arrival at the hospital will typically have maximal tenderness over the medial aspect of the upper patella, reflecting damage to the attachment of the vastus medialis. There may be ‘apprehension’ when gentle lateral pressure is applied to the patella. If clinical features are dramatic, rest in a splint (occasionally, cylinder POP may be needed); otherwise refer for physiotherapy and orthopaedic follow- up.
Dislocation of the knee
- Although rare, this injury indicates severe disruption of the ligamentous structures and soft tissues of the knee. Look carefully for associated injuries (e.g. femur or lower limb), and document distal pulses and sensation— the popliteal artery or nerve are often injured.
- Reduction requires adequate (IV opioid) analgesia and usually GA or sedation with full precautions.
- Reduce by simple traction on the limb, correcting the deformity. Check distal pulses and sensation after reduction; immobilise in a long leg POP backslab, and arrange orthopaedic admission.
- Check the circulation repeatedly, since popliteal artery damage may not become apparent for some hours— angiography is usually required. Compartment syndrome is another recognised complication.
Tibial plateau fracture
- Falls onto an extended leg can cause compression fractures of the proximal tibia. Valgus stresses crush or fracture the lateral tibial plateau. These injuries are commonly seen in pedestrians injured following impact with car bumpers. Varus injuries result in crushing or fracture of the medial tibial plateau and are usually associated with rupture of the opposite collateral ligaments.
- Examine for tenderness over the medial or lateral margins of the proximal tibia. Look for swelling, haemarthrosis, or ligamentous instability.
- Look carefully on X- rays for breaks in the articular surfaces of the proximal tibia, avulsions from the ligamentous attachments, or loss of height from the medial and lateral tibial plateau, but beware this may be subtle. Adopt a low threshold to request a CT scan to clarify the nature and extent of the injury. Lipohaemarthrosis results from an intra-articular fracture with escape of fat and blood from the bone marrow into the joint, and is most frequently seen in the knee, associated with a tibial plateau fracture or distal femoral fracture; rarely a patellar fracture. The fatty marrow separates from the water-based blood and layers above it, forming a fat-fluid level.
- Treat with immobilisation in a long leg POP backslab, following adequate analgesia, and refer to orthopaedics. Fractures of the tibial plateau often require elevation ± ORIF with bone grafting. Admit all patients with acute haemarthrosis. Treat small, isolated avulsions without haemarthrosis with immobilisation, crutches, and analgesia, and arrange orthopaedic follow-up.
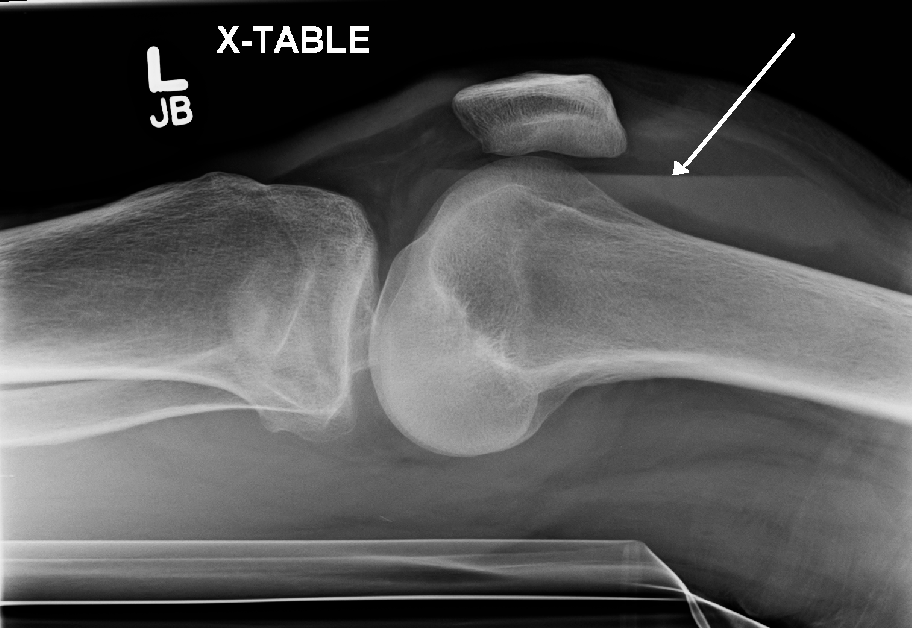
Lipohaemarthrosis in a patient with a subtle tibial plateau fracture. (Image by James Heilman, MD (Own work) [CC BY-SA 3.0 , via Wikimedia Commons)
Posterolateral corner injuries
- The posterolateral corner of the knee comprises a group of ligaments and muscles/tendons that add to the stability of the joint. Posterolateral corner injuries often occur in association with other significant knee trauma (e.g. dislocations, rupture of anterior or posterior cruciate ligaments), but isolated injuries can occur.
- Suspect this injury when significant symptoms follow the application of varus force to the anteromedial aspect of the extended knee. Chronic instability can result.
- X- rays may be normal or show subtle avulsions or widening of the lateral joint space.
- Urgent MRI and orthopaedic referral will enable prompt treatment.
Acute haemarthrosis
- Rapid- onset swelling following a knee injury, often warm, tense, and painful.
- Common causes include cruciate ligament rupture, tibial avulsion, and tibial plateau or other fractures. An acute haemarthrosis indicates serious injury.
- Refer for orthopaedic appraisal following splintage, analgesia, and appropriate X- rays. Aspiration of a haemarthrosis (advocated by some experts to provide analgesia) requires a strict aseptic technique.
Cruciate ligament rupture
- Pain and swelling can make it hard to elicit classical physical signs. An audible ‘pop’ at the time of injury is highly suggestive of anterior cruciate ligament rupture. Anterior cruciate ligament tears often occur in association with tears of the medial collateral ligament and/ or medial meniscus.
- Examine for the presence of haemarthrosis, abnormal increased anterior glide of the tibia (‘+ve anterior drawer test’), and injuries to the medial collateral ligament or other structures.
- Look carefully at X- rays for avulsion of the anterior tibial spine (anterior cruciate insertion).
- Give analgesia, and refer to the orthopaedic surgeon.
- In posterior cruciate ligament tears, the tibia may appear to sag back when the knee is flexed, so the tibia can be pulled into a more normal position, causing a ‘false +ve’ anterior drawer test. X- rays may reveal the relevant posterior tibial spine to be avulsed. Provide analgesia and refer.
Collateral ligament injuries
- Tenderness over the medial or lateral collateral ligament, with pain at this site on stress testing, indicates collateral ligament injury.
- Most injuries are isolated and have no associated haemarthrosis and no abnormality on X- ray.
- The degree of laxity on stress testing will help to guide treatment:
- Local tenderness with no laxity (or very slight laxity) implies a grade I injury. Treat with analgesia and physiotherapy (± crutches), with an expectation of full recovery in 2– 4 weeks.
- Local tenderness with minor/ moderate laxity, but with a definite end- point, implies a grade II injury. Provide analgesia, crutches, and instruction on quadriceps exercises, and refer for orthopaedic follow- up.
- Major laxity (i.e. the joint opening up >1cm) with no end- point implies complete rupture. Consider a POP cylinder (or splint), and provide crutches, analgesia, quadriceps exercises, and orthopaedic follow- up.
Ruptured quadriceps tendon
- Complete rupture of the distal quadriceps insertion can result from a direct injury or from sudden, violent contraction of the quadriceps muscle.
- Examination reveals complete inability to straight leg raise— never assume this is just due to pain. There may be a palpable defect in the muscle insertion.
- Refer to the orthopaedic surgeon for repair.
Ruptured patellar tendon
- Examine for complete inability to straight leg raise and a high-riding patella, a palpable defect in the patellar tendon.
- There is frequently an associated avulsion of the tibial tuberosity.
- Refer to orthopaedics for repair.
Acutely locked knee
- A springy block to full extension (which varies from just a few degrees to much more) in the knee indicates an underlying meniscal injury or other loose body in the knee joint.
- Obtain knee X- rays (including a tunnel view), which may show a loose body.
- Do not attempt to unlock the knee by manipulation, as this is usually painful and futile. Give analgesia, and refer for arthroscopy.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |