

Trauma

A 21 year old male is brought into the Emergency Department with burns following an accident with a firework. The burns cover the right half of the anterior trunk and two/thirds of the right upper limb. What is the total burn surface area (TBSA)?
Answer:
The adult body configuration is divided into anatomic regions that represent multiples of 9%:- Upper limb – 9%
- Head – 9%
- Lower limb – 18%
- Anterior trunk - 18%
- Posterior trunk – 18%
- Groin - 1%
Burns: Assessment and Management
Trauma
Last Updated: 7th December 2023
Assessment of burns
Body surface area
The rule of nines is a practical guide for determining the extent of a burn using calculations based on areas of partial- and full-thickness burns. The rule of nines helps estimate the extent of burns with irregular outlines or distribution and is the preferred tool for calculating and documenting the extent of a burn injury. The adult body configuration is divided into anatomic regions that represent multiples of 9%:
- Upper limb – 9%
- Head – 9%
- Lower limb – 18%
- Anterior trunk - 18%
- Posterior trunk – 18%
- Groin - 1%
The palmar surface (including the fingers) of the patient’s hand represents approximately 1% of the patient’s body surface. These figures are used to calculate the total body surface area (TBSA) affected by burns.
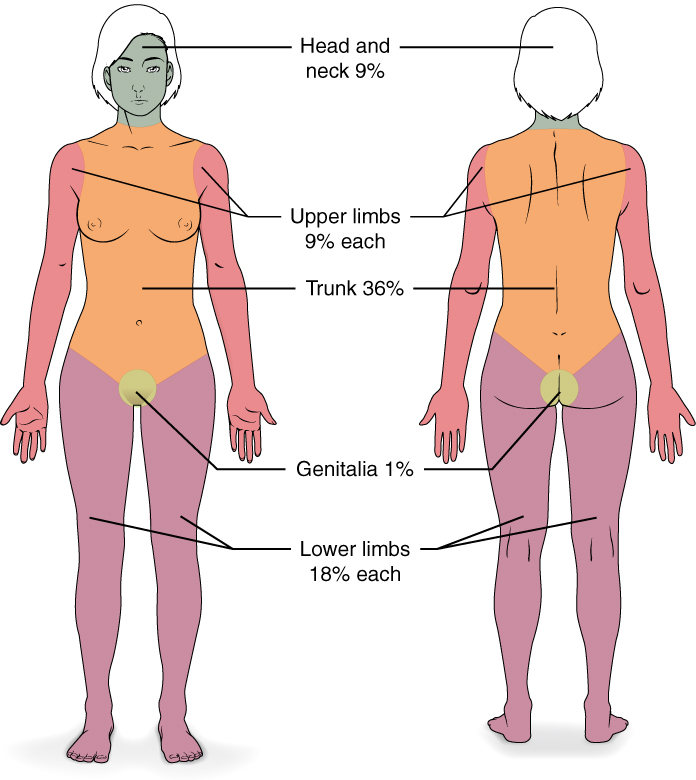
Rule of Nines. (Image by OpenStax College, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons)
Depth of burn
| Depth of burn | Layers affected | Clinical findings |
|---|---|---|
| Superficial epidermal | Epidermis | Skin is erythematous and painful but not blistered and blanches to touch |
| Superficial partial thickness | Extends into superficial (papillary) dermis | Skin is moist, painfully hypersensitive (even to air current), blistered, homogeneously pink, and blanches to touch |
| Deep partial thickness | Extends into deep (reticular) dermis | Skin is typically drier, less painful (only to pressure), potentially blistered, red or mottled in appearance, and blanches with a sluggish return or does not blanch with pressure |
| Full thickness | Extends through entire dermis and into subcutaneous tissue | Skin may appear translucent or waxy white, or brown and leathery, with no blisters, the surface is painless and generally dry, and does not blanch with pressure |
General management of burns
Gastric tube insertion
- To prevent vomiting and possible aspiration in patients with nausea, vomiting, or abdominal distention, or when a patient’s burns involve more than 20% total BSA, insert a gastric tube and ensure it is functioning before transferring the patient.
Analgesics and sedatives
- Severely burned patients may be restless and anxious from hypoxaemia or hypovolaemia rather than pain. Consequently, manage hypoxaemia and inadequate fluid resuscitation before administering opioid analgesics or sedatives, which can mask the signs of hypoxaemia and hypovolaemia.
- Opioid analgesics and sedatives should be administered in small, frequent doses by the intravenous route only. Remember that simply covering the wound will decrease the pain.
Wound care
- Wound cleaning
- Cleansing is useful for removing foreign bodies, soluble debris, excess slough, or necrotic tissue, which may become a focus for infection.
- Cleansing is advised prior to obtaining a bacteriology swab (but do not take swabs unless there is clinical evidence of wound infection).
- If a clean technique is being used, use lukewarm tap water. If a sterile technique is required, use 0.9% normal saline.
- Ideally, the cleansing fluid should be at body temperature, or if this is not possible, the fluid should be warmed to room temperature before use.
- Gentle wound irrigation
- Do not clean wounds by scrubbing, which causes pain and local tissue oedema. Irrigation is more protective of fragile tissue.
- Do not use topical antiseptics due to reported pain, tissue damage, wound drying, and delayed healing.
- Gentle debridement
- Debridement describes the removal of necrotic, devitalized, sloughy, or infected tissue. This allows visualisation of the wound bed and may encourage epithelialisation. Specialist surgical debridement may be appropriate following referral.
- Blister management
- Blisters should be left intact wherever possible, to reduce the risk of infection.
- Consider de-roofing large blisters (for example, greater than 1 cm2); blisters that are likely to rupture or are over a joint, using an aseptic technique.
- Wound dressing
- The choice of dressing will depend on the site, size, and depth of the wound, level of exudate, infection risk, and on local formulary availability.
- Ensure that all individuals who come into contact with the wound wear gloves and a gown, and minimise the number of caregivers within the patient’s environment without protective gear.
Antibiotics
- There is no indication for prophylactic antibiotics in the early postburn period. Reserve use of antibiotics for the treatment of infection.
Tetanus
- Determination of the patient’s tetanus immunisation status and initiation of appropriate management is very important.
Management of specific burn injuries
Circumferential extremity burns
- The goal of assessing peripheral circulation in a patient with burns is to rule out compartment syndrome.
- Compartment syndrome results from an increase in pressure inside a compartment that interferes with perfusion to the structures within that compartment. In burns, this condition results from the combination of decreased skin elasticity and increased oedema in the soft tissue.
- In extremities, the main concern is perfusion to the muscle within the compartment. Although a compartment pressure greater than systolic blood pressure is required to lose a pulse distal to the burn, a pressure of > 30 mm Hg within the compartment can lead to muscle necrosis. Once the pulse is gone, it may be too late to save the muscle.
- Thus, clinicians must be aware of the signs and symptoms of compartment syndrome:
- Pain greater than expected and out of proportion to the stimulus or injury
- Pain on passive stretch of the affected muscle
- Tense swelling of the affected compartment
- Paraesthesias or altered sensation distal to the affected compartment
- A high index of suspicion is necessary when patients are unable to cooperate with an exam.
- Compartment syndromes may also present with circumferential chest and abdominal burns, leading to increased peak inspiratory pressures or abdominal compartment syndrome.
- Chest and abdominal escharotomies performed along the anterior axillary lines with a cross-incision at the clavicular line and the junction of the thorax and abdomen usually relieve the problem.
- To maintain peripheral circulation in patients with circumferential extremity burns, the clinician should:
- Remove all jewellery and identification or allergy bands on the patient’s extremities.
- Assess the status of distal circulation, checking for cyanosis, impaired capillary refill, and progressive neurologic signs such as paraesthesia and deep-tissue pain. Assessment of peripheral pulses in patients with burns is best performed with a Doppler ultrasonic flow meter.
- Relieve circulatory compromise in a circumferentially burned limb by escharotomy, always with surgical consultation. Escharotomies usually are not needed within the first 6 hours of a burn injury.
- Although fasciotomy is seldom required, it may be necessary to restore circulation in patients with associated skeletal trauma, crush injury, or high-voltage electrical injury.
- Although standard escharotomy diagrams are generally followed, always attempt to incise the skin through the burned, not the unburned skin (if unburned skin is present), as the burned skin will likely be debrided by the burn center.
Chemical burns
- Chemical injury can result from exposure to acids, alkalies, and petroleum products.
- Acidic burns cause a coagulation necrosis of the surrounding tissue, which impedes the penetration of the acid to some extent.
- Alkali burns are generally more serious than acid burns, as the alkali penetrates more deeply by liquefaction necrosis of the tissue.
- Rapid removal of the chemical and immediate attention to wound care are essential. Chemical burns are influenced by the duration of contact, concentration of the chemical, and amount of the agent.
- If dry powder is still present on the skin, brush it away before irrigating with water. Otherwise, immediately flush away the chemical with large amounts of warmed water, for at least 20 to 30 minutes, using a shower or hose. Alkali burns require longer irrigation.
- Neutralising agents offer no advantage over water lavage, because reaction with the neutralising agent can itself produce heat and cause further tissue damage.
- Alkali burns to the eye require continuous irrigation during the first 8 hours after the burn. A small-caliber cannula can be fixed in the palpebral sulcus for irrigation.
- Certain chemical burns (such as hydrofluoric acid burns) require specialised burn unit consultation. It is important to ascertain the nature of the chemical and if possible obtain a copy of the Material Safety Data Sheet to address any systemic toxicity that may result. Providers must also take care to protect themselves from inadvertent exposure during the decontamination process.
Electrical burns
- Electrical burns result when a source of electrical power makes contact with a patient, and current is transmitted through the body. The body can also serve as a volume conductor of electrical energy, and the heat generated results in thermal injury to tissue.
- Different rates of heat loss from superficial and deep tissues allow for relatively normal overlying skin to coexist with deep-muscle necrosis. Therefore, electrical burns frequently are more serious than they appear on the body surface, and extremities, particularly digits, are especially at risk. In addition, the current travels inside blood vessels and nerves and can cause local thrombosis and nerve injury.
- Severe electrical injuries usually result in contracture of the affected extremity. A clenched hand with a small electrical entrance wound should alert the clinician that a deep soft-tissue injury is likely much more extensive than is visible to the naked eye.
- Patients with severe electrical injuries frequently require fasciotomies and should be transferred to burn centers early in their course of treatment.
- Immediate treatment of a patient with a significant electrical burn includes establishing an airway and ensuring adequate oxygenation and ventilation, placing an intravenous line in an uninvolved extremity, ECG monitoring, and placing an indwelling bladder catheter.
- Electricity can cause cardiac arrhythmias that may produce cardiac arrest. Prolonged monitoring is reserved for patients who demonstrate injury from the burn, loss of consciousness, exposure to high voltage (>1,000 volts) or cardiac rhythm abnormalities or arrhythmias on early evaluation.
- Because electricity causes forced contraction of muscles, clinicians need to examine the patient for associated skeletal and muscular damage, including the possibility of fracture of the spine.
- Rhabdomyolysis from the electricity traveling through muscle results in myoglobin release, which can cause acute renal failure. Do not wait for laboratory confirmation before instituting therapy for myoglobinuria. If the patient’s urine is dark red, assume that haemochromogens are in the urine.
- ABA consensus formula guidelines are to start resuscitation for electrical burn injury at 4 mL/kg/%TBSA to ensure a urinary output of 100 mL/hr in adults. Once the urine is clear of pigmentation, titrate the IV fluid down to ensure a standard urine output of 0.5 mL/kg/hr.
- Consult a local burn unit before initiating a bicarbonate infusion or using mannitol.
Tar burns
- In industrial settings, individuals can sustain injuries secondary to hot tar or asphalt. The temperature of molten tar can be very high—up to 450°F (232°C)— if it is fresh from the melting pot. A complicating factor is adherence of the tar to skin and infiltration into clothing, resulting in continued transfer of heat.
- Treatment includes rapid cooling of the tar and care to avoid further trauma while removing the tar. A number of methods are reported in the literature; the simplest is use of mineral oil to dissolve the tar. The oil is inert, safe on injured skin, and available in large quantities.
Patient transfer
The criteria for transfer of patients to burn centers has been developed by the American Burn Association. The following types of burn injuries typically require transfer to a burn center:
- Partial-thickness burns on greater than 10% TBSA
- Burns involving the face, hands, feet, genitalia, perineum, and major joints
- Third-degree (full-thickness) burns in any age group
- Electrical burns, including lightning injury
- Chemical burns
- Inhalation injury
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality (e.g. diabetes, renal failure)
- Any patient with burns and concomitant trauma (e.g. fractures) in which the burn injury poses the greatest risk of morbidity or mortality
- Burned children in hospitals without qualified personnel or equipment for the care of children
- Burn injury in patients who will require special social, emotional, or rehabilitative intervention
Because these criteria are so comprehensive, clinicians may elect to consult with a burn center and determine a mutually agreeable plan other than transfer. For example, in the case of a partial thickness hand or face burn, if adequate wound care can be taught and oral pain control tolerated, follow-up at an outpatient burn clinic can avoid the costs of immediate transfer to a burn center.
Complications of burns
- Early complications
- Respiratory distress (smoke inhalation or a circumferential chest burn)
- Poisoning from inhalation of noxious gases released by burning
- Fluid loss, hypotension, and hypovolaemic shock
- Hypothermia (epidermal damage may lead to problems with thermoregulation)
- Wound infection and sepsis
- Toxic shock syndrome (complication of infection caused by S.aureus)
- Cardiac arrhythmias (electrical shock or electrolyte disturbance)
- Vascular insufficiency, distal ischaemia, or compartment syndrome (from circumferential burn of limb or digit)
- Acute kidney injury (from rhabdomyolysis)
- Limb loss
Death
- Late complications
- Wound infection
- Chronic neuropathic pain and itch
- Scarring
- Contractures
- Psychosocial impact
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |