

Trauma
Question 47 of 216

A 72 year old man is brought to the Emergency Department after falling at home. He is complaining of pain to the left hip. What is the diagnosis?
Answer:
- Intracapsular femoral neck fractures are graded according to the Garden classification.
-
- Garden I: Trabeculae angulated, but inferior cortex intact. No significant displacement
- Garden II: Trabeculae in line, but a fracture line visible from superior to inferior cortex. No significant displacement
- Garden III: Obvious complete fracture line, with slight displacement and/ or rotation of the femoral head
- Garden IV: Gross, often complete, displacement of the femoral head
Hip and Thigh Injuries
Trauma
Last Updated: 31st January 2023
Acetabular fracture
- Often accompanies traumatic hip dislocation following violent injury e.g. RTA.
- May follow fall in elderly patients with osteoporosis.
- Posterior rim fractures are the most common.
- Complications include massive haemorrhage, sciatic nerve damage, myositis ossificans, and secondary osteoarthritis.
- Resuscitate, give analgesia, and deal with priorities first.
- CT demonstrates the exact injury better than X- ray.
- Refer to orthopaedics.
Posterior hip dislocation
- Implies major trauma, often with other critical injuries (e.g. dashboard knee injury in a car crash) or fractured posterior acetabulum.
- The limb is shortened and internally rotated, with the hip flexed and adducted. This appearance may be absent if there is also a femoral shaft fracture.
- Check for sciatic nerve damage— examine foot dorsiflexion and below-knee sensation.
- Complications: sciatic nerve injury, avascular necrosis of the femoral head (risk increases the longer the hip is dislocated), and secondary OA.
- Resuscitate, give analgesia, and address ABC priorities. Refer for reduction under GA. In unconscious or anaesthetised patients, reduce in the ED.
- Reduction technique for posterior dislocation (‘Allis technique’)
- It is easiest and safest to reduce dislocation if the anaesthetised patient is placed on the floor. If this is not possible, stand on the trolley. An assistant presses down on the patient’s anterior superior iliac spines to hold down the pelvis.
- Flex the hip and knee, both to 90°, and correct adduction and internal rotation deformities.
- Grip the patient’s lower leg between your knees, and grasp the patient’s knee with both hands.
- Lean back and lever the knee up, pulling the patient’s hip upward. A ‘clunk’ confirms successful reduction. X- ray to confirm reduction.
Anterior hip dislocation
- Less common.
- The leg is held abducted and externally rotated.
- Complications include damage to the femoral nerve, artery, and vein.
- Give analgesia and refer for reduction under GA.
Dislocated hip prosthesis
- Relatively common (affects 73% of total hip replacements). It can follow minor (or even no) trauma— sometimes, crossing legs or flexing the hip to 90° can be enough.
- The patient presents in severe pain, unable to move the hip. Confirm posterior dislocation of the hip prosthesis by X- ray.
- Give IV opioid, and refer to orthopaedics for MUA (and assessment of prosthesis stability) under GA. Depending on protocols, expertise, and resources (especially for recovery), it may be possible to do this in the ED.
Neck of femur fracture classification
- Intracapsular fracture
- Subcapital (below the femoral head)
- Transcervical (across the mid-femoral neck)
- Basicervical (across the base of the femoral neck)
- Extracapsular fracture
- Intertrochanteric (between the trochanters)
- Pertrochanteric (involves the trochanters)
- Subtrochanteric (distal to the trochanters)
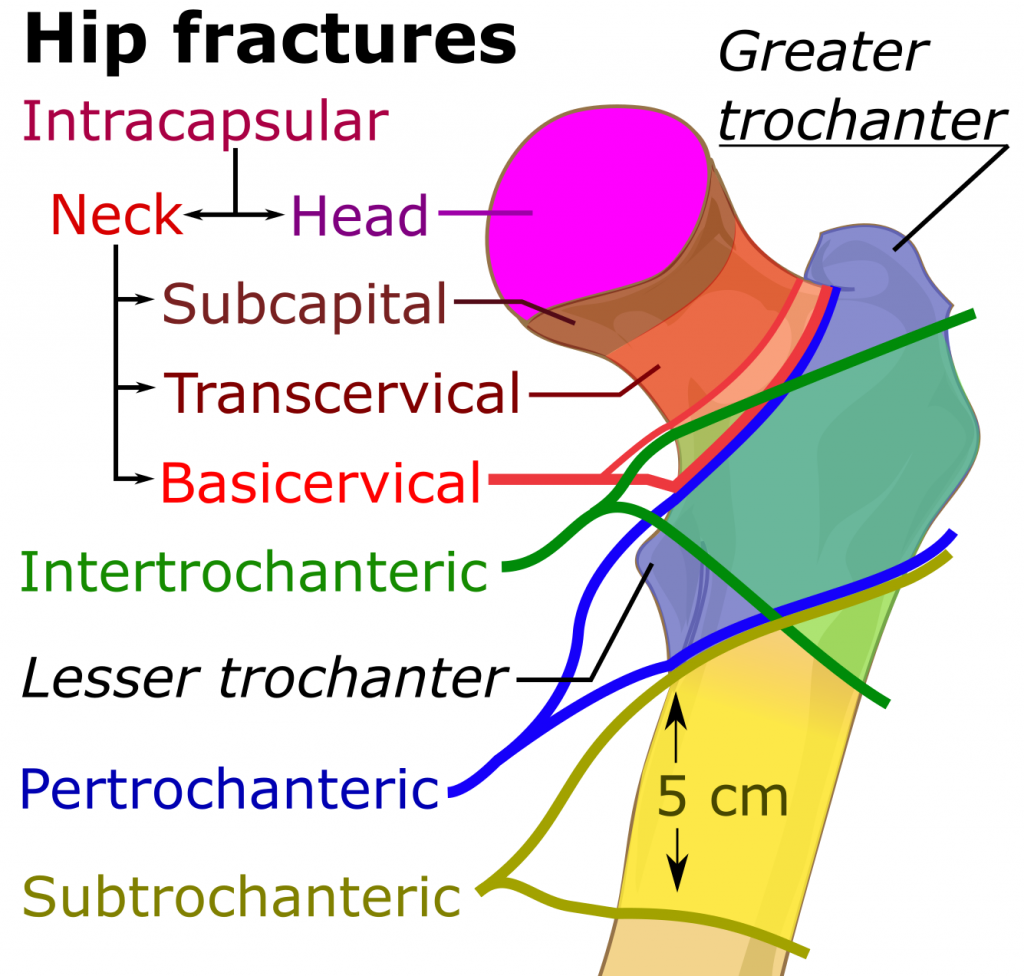
Proximal femur fractures. (Image by Mikael Häggström, using image by Mariana Ruiz Villarreal (LadyofHats [CC0], via Wikimedia Commons)
Intracapsular fractures of neck of femur
- Mechanism of injury
- Can follow relatively minor trauma.
- Risk increases in the elderly, because of osteoporosis, osteomalacia, and increased rate of falls. These fractures can disrupt the blood supply to the femoral head, causing avascular necrosis.
- Fractures around the hip in younger patients imply high- energy injury— the incidence of non-union or avascular necrosis may be as high as 20%.
- Clinical features
- Usually follows a fall onto the hip or bottom.
- Pain may radiate down towards the knee.
- The affected leg may be shortened and externally rotated.
- Check for hypothermia and dehydration (the patient may have been lying for hours).
- Look for tenderness over the hip, particularly on rotation.
- Suspect hip fracture in an elderly person who:
- Exhibits a sudden inability to weight- bear. There may be no history of injury, particularly in the presence of confusion or dementia.
- Is unable to weight- bear and has pain in the knee (the hip may not be painful).
- Has ‘gone off her feet’.
- Diagnosis
- Look closely for disrupted trabeculae/ cortices and abnormal pelvic contours (Shenton’s lines).
- Fractures of the femoral neck are not always visible on initial X- rays. Repeat X- rays, CT, or MRI may be required if symptoms continue.
- Intracapsular femoral neck fractures are graded according to the Garden classification.
- Garden I: Trabeculae angulated, but inferior cortex intact. No significant displacement
- Garden II: Trabeculae in line, but a fracture line visible from superior to inferior cortex. No significant displacement
- Garden III: Obvious complete fracture line, with slight displacement and/ or rotation of the femoral head
- Garden IV: Gross, often complete, displacement of the femoral head
- ED management
- Obtain IV access and send blood for U&E, glucose, FBC, and cross- match.
- Start IVI if indicated (e.g. dehydration or shock).
- Assess patient's pain immediately on presentation at hospital, within 30 minutes of administering initial analgesia and hourly until settled on ward.
- Offer immediate analgesia to patients presenting at hospital with suspected hip fracture, including people with cognitive impairment.
- Offer paracetamol every 6 hours preoperatively unless contraindicated. Offer additional opioids if paracetamol alone does not provide sufficient pain relief. Non-steroidal anti-inflammatory drugs (NSAIDs) are not recommended.
- Consider adding nerve blocks if paracetamol and opioids do not provide sufficient preoperative pain relief, or to limit opioid dosage (e.g. fascia iliaca block)
- Obtain an ECG to look for arrhythmias/ MI, and consider the need for CXR.
- Arrange other investigations as indicated by the history/ examination.
- Admit to the orthopaedic ward.
- Orthopaedic management
- Perform surgery on the day of, or the day after, admission.
- Identify and treat correctable comorbidities immediately so that surgery is not delayed.
- Offer patients a choice of spinal or general anaesthesia after discussing the risks and benefits. Consider intraoperative nerve blocks for all patients undergoing surgery.
- Offer replacement arthroplasty (total hip replacement or hemiarthroplasty) to patients with a displaced intracapsular hip fracture.
- Consider total hip replacement rather than hemiarthroplasty for people with a displaced intracapsular hip fracture who:
- were able to walk independently out of doors with no more than the use of a stick and
- do not have a condition or comorbidity that makes the procedure unsuitable for them and
- are expected to be able to carry out activities of daily living independently beyond 2 years.
- Use extramedullary implants such as a sliding hip screw in preference to an intramedullary nail in people with trochanteric fractures above and including the lesser trochanter (except reverse oblique).
- Use an intramedullary nail to treat patients with a subtrochanteric fracture.
- Hip pain after injury with no fracture seen
- Elderly patients who report hip pain and struggle to walk after a fall, and yet have no fracture of the hip or pubic rami on X- ray, may need assessment by an occupational therapist or physiotherapist before deciding if they can be safely discharged home with analgesia and appropriate walking aid. A small, but significant, proportion of such patients will turn out to have a hip fracture.
- Offer magnetic resonance imaging (MRI) if hip fracture is suspected despite negative X-rays of the hip of an adequate standard. If MRI is not available within 24 hours or is contraindicated, consider computed tomography (CT).
- For patients who have normal X- rays, are able to mobilise satisfactorily, and are being discharged, advise them to return for review and further imaging (CT or MRI) if the pain continues for >1 week— ideally, provide an advice leaflet to explain and reinforce this.
- Complications
- Infection
- Haemorrhage
- Avascular necrosis
- Delayed union, malunion and non-union
- Venous thromboembolism
- Pneumonia
- Pressure ulcers
Extracapsular fractures of neck of femur
- Intertrochanteric
- These affect the base of the femoral neck and the intertrochanteric region. Initial management is identical to that for neck of femur fractures.
- Isolated trochanteric avulsion fracture
- Sudden force may avulse insertions of the gluteus medius (greater trochanter) or iliopsoas (lesser trochanter). Give analgesia; assess mobility with crutches, and refer for follow- up for gradual mobilisation and symptomatic treatment.
- Subtrochanteric
- These involve the most proximal part of the femoral shaft, at or just distal to the trochanters. They typically involve high- energy trauma in younger patients and are often associated with other serious injuries. They can also occur as isolated injuries following relatively minor trauma in those with osteoporosis or metastatic disease. Treat as for femoral shaft fractures.
Shaft of femur fracture
- Mechanism of action
- Enormous force is required to break an undiseased adult femoral shaft. Fractures are frequently associated with multisystem trauma. Treatment of immediately life- threatening injuries takes priority. Transverse, spiral, or segmental shaft fractures usually result from falls, crushing injuries, or high- speed road traffic collisions. There is often associated dislocation of the hip or other serious injury to the lower limb ± major trauma affecting the head, chest, abdomen, and pelvis.
- Complications
- Closed fractures of the femoral shaft, even without obvious vascular injury, may be associated with marked blood loss. Up to 1.5L of blood may be lost without visible thigh swelling. Rarely, gross blood loss may occur from compound femoral fractures. Later complications include fat embolism/ ARDS. The incidence of complications is decreased by early splintage and early definitive treatment (usually closed intramedullary nailing).
- Clinical features
- The diagnosis is usually clear on examination, with deformity, shortening, external rotation, and abduction at the hip on the affected side. The fracture may be felt or even heard on movement of the lower limb. Carefully check for associated pelvic, knee, or distal limb injuries or for the presence of associated wounds. Document sensation and pulses in the limb, and recheck frequently.
- Management
- Before X- rays, resuscitate, exclude life- threatening injuries, replace IV fluids, give adequate analgesia, and splint fractures as follows:
- Assess ABC, establish priorities, and resuscitate as for patients presenting with major trauma.
- Commence fluid replacement via two large- bore IV cannulae— start with 1000mL of 0.9% saline.
- Obtain blood for cross- matching, plus U&E, FBC, and coagulation screen.
- Administer IV analgesia— give small increments of opioid (with an antiemetic) until pain is controlled.
- Give IV tranexamic acid
- Strongly consider femoral nerve block or fascia iliaca block. As this starts to take effect (~5– 10min), prepare splintage and immobilise in a traction splint (e.g. Kendrick).
- Arrange imaging of the femur— very often a trauma pan- CT scan of the head, neck, chest, abdomen, and pelvis can be appropriately extended down to involve the femoral shafts.
- Before X- rays, resuscitate, exclude life- threatening injuries, replace IV fluids, give adequate analgesia, and splint fractures as follows:
Supracondylar femoral fractures
- Fractures of the distal third of the femur usually follow violent direct force.
- They are frequently comminuted and often intra- articular with associated damage to the knee joint. In adults, the distal femoral fragment tends to rotate due to pulling from the gastrocnemius.
- Treat as for femoral shaft fractures, but note that femoral nerve block may not be as effective.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |