

Trauma
This was previously featured in an exam
A 10 year old child presents to ED with bilateral burns to her forearms after pulling a pan of hot water off the stove. She is distressed and in severe pain. Your ED does not have a local burns centre. Which of the following is the first line analgesia for this patient?
Answer:
- Analgesia
- Most burned children will be severe pain and this should be dealt with urgently.
- Some older children may manage to use Entonox but most will not.
- Any child with more than a minor burn should be given intranasal diamorphine initially and then further pain can be controlled with intravenous morphine at a dose of 100 micrograms/kg (< 1 year: 80 micrograms/kg), if needed, as soon as possible.
- Further doses are often required but must be titrated against pain and sedation.
Paediatric Burns
Trauma
Last Updated: 24th February 2026
Primary survey and resuscitation
- Airway
- May be compromised either because of inhalational injury and oral scalds or because of severe burns to the face
- Indications of inhalational injury
- History of exposure to smoke in a confined space
- Deposits around the mouth and nose
- Carbonaceous sputum
- Any suspicion of airway compromise, or the discovery of injuries that might be expected to cause problems with the airway at a later stage, should lead to immediate consideration of tracheal intubation.
- Breathing
- Signs that should arouse suspicion of inadequacy of breathing include abnormal rate, abnormal chest movements, and cyanosis (a late sign).
- Circumferential burns to the chest or abdomen (in infants) may cause breathing difficulties by mechanically restricting chest wall movement.
- All children who have suffered significant burns should be given high-flow oxygen. If there is evidence of increased work of breathing then senior anaesthetic help should be sought and intubation and ventilation should be considered.
- Circulation
- In the first few hours following injury signs of hypovolaemic shock are rarely attributable to burns; therefore any such signs should arouse suspicion of an alternative cause.
- Intravenous access be established with two cannulae during resuscitation, and fluids started. Blood should be taken for blood glucose, carboxyhaemoglobin level, haemoglobin, urea and electrolytes and cross-matching at this stage.
- Disability
- Reduced conscious level following burns may be due to hypoxia, head injury or hypovolaemia.
- Exposure
- Exposure should be complete remembering that burned children lose heat quickly and should be kept in a warm environment and covered with blankets when not being examined.
Burn assessment
The severity of a burn depends on its relative surface area and depth, and on its location.
Surface area:
Surface area is usually estimated using burns charts. It is particularly important to use a paediatric chart when assessing burn size in children because the relative surface areas of the head and limbs change with age. Another useful method of estimated surface area relies on the fact that the patient's palm and adducted fingers cover an area of approximately 1% of the body surface. This method can be used when charts are not immediately available. Note that the 'rule of 9s' cannot be used in a child who is under 14 years of age.
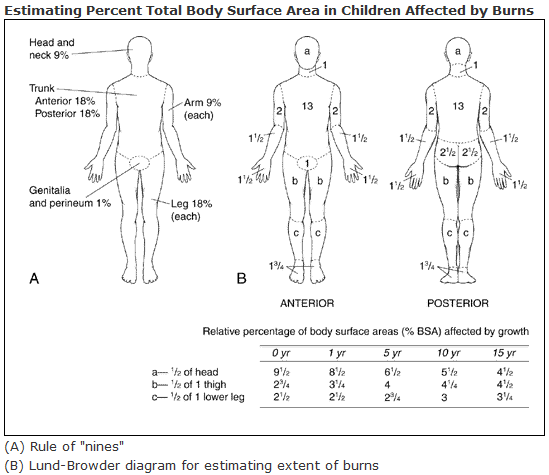
Burn Assessment. (Image by U.S. Department of Health and Human Services ) [Public domain], via Wikimedia Commons)
- Superficial epidermal
- Superficial dermal - pale pink skin with blisters
- Mid-dermal - sluggish capillary refill, dark pink in colour, decreased sensation to touch
- Deep dermal - blotchy red skin, +/- blisters, loss of capillary blush phenomenon
- Partial thickness - blistering, skin is pink or mottled
- Full thickness - white or charred in colour, painless and leathery to the touch
Special areas:
- Burns to the face and mouth can cause airway obstruction.
- Burns involving the hands and feet can cause severe functional loss if scarring occurs.
- Perineal burns are prone to infection and present specific management problems.
- Circumferential, full- or partial- thickness burns of the limbs or neck may require urgent incision to relieve distal ischaemia.
- Circumferential burns of the chest may restrict ventilation and require escharotomy.
Emergency treatment
- Analgesia
- Most burned children will be severe pain and this should be dealt with urgently.
- Some older children may manage to use Entonox but most will not.
- Any child with more than a minor burn should be given intranasal diamorphine initially and then further pain can be controlled with intravenous morphine at a dose of 100 micrograms/kg (< 1 year: 80 micrograms/kg), if needed, as soon as possible.
- Further doses are often required but must be titrated against pain and sedation.
- Fluid therapy
- Two cannulae should have already been sited during the primary survey and resuscitation and therapy for shock (10 + 10 mL/kg) commenced if indicated.
- Children with burns of 10% body surface area or more will require intravenous fluids as part of their burns care (this is in addition to their normal fluid requirement).
- The additional fluid required per day to treat the burn is estimated using the modified Parkland formula: Percentage burn x Weight (kg) x 3ml
- Half of this fluid should be given in the first 8 hours following the time of the burn. The fluid given is usually crystalloid.
- Subsequent therapy is guided by urine output, which should be kept at 1 ml/kg/h or more (in children who have sustained greater than 15% TBSA burns, it should be 2 ml/kg/h).
- Urethral catheterisation should be considered early to help with fluid management.
- Wound care
- Wound care should be started as early as possible to reduce risk of infection and reduce pain.
- The burned area should be cooled immediately for 20 minutes. Cold compresses and irrigation with cold water can be used but should be used with caution as burned children lose heat rapidly.
- Burns should then be covered with non-adhesive sterile towels. Cling film can be used as a sterile dressing and can be applied loosely onto the burned area. Blisters should be left intact.
- Provide tetanus prophylaxis if required.
Management of carbon monoxide poisoning
During a fire, burning of organic compounds in a low-oxygen environment produces carbon monoxide. Inhalation by the victim induces the production of carboxyhaemoglobin, which has a 200-fold greater affinity for the oxygen molecule than haemoglobin. A high-level will therefore cause cellular hypoxia, as oxygen will not be given up to the cells. Children who have been in house fires should have their blood carboxyhaemoglobin measured. Normal SpO2 does not exclude carbon monoxide poisoning. Levels of 5 - 20% are treated with high flow oxygen which speeds up the removal of carbon monoxide. Levels over 20% should prompt consideration of hyperbaric oxygen chamber treatment - discuss with the paediatrics burn service.
In some environments, the burning of plastics, wool and silk can produce cyanide. Assessment and treatments are complex. Be aware of the possibility of cyanide poisoning and consider it in a child from a house fire who is in a coma or prevents with a severe metabolic acidosis without apparent cause. In general, antidotes are used when blood levels of cyanide are greater than 3 mg/L. Discuss treatment immediately with a poisons centre.
Transfer to definitive care
Initial indication for referral to a specialised burns service (as per APLS):
- A child with a partial-thickness burn ≥ 2% total body surface area (TBSA)
- In addition, any child with a burn injury regardless of age and %TBSA who presents with any of the following should be discussed with the local burns service:
- Inhalation injury
- Full-thickness burn ≥ 1% TBSA
- Burns to special areas (hands, face, neck, feet, perineum)
- Burns to area involving a joint that may affect mobility and function
- Electrical burns
- Chemical burns
- Any burn with suspicion of non-accidental injury
- Burns associated with major trauma
- Burns associated with significant comorbidities
- Circumferential burns to the trunk or limbs
Suspecting non-accidental injury in children with burns
- Suspect non-accidental injury if a child or adult has a burn or scald with any of the following:
- Explanation for the injury is absent or unsuitable.
- The person is not independently mobile.
- The injury is on any soft tissue area that would not be expected to come into contact with a hot object in an accident (for example, the backs of hands, soles of feet, buttocks, back).
- The injury is in the shape of an implement (for example, cigarette, iron in contact burns).
- The injury indicates forced immersion, for example, scalds:
- To the buttocks, perineum, and lower limbs.
- To limbs in a glove or stocking distribution.
- To limbs with a symmetrical distribution.
- With sharply delineated borders.
- Consider the possibility of non-accidental injury if there is:
- Delayed presentation in seeking medical attention. Note: this may be due to effective first aid measures masking the severity of the injury.
- An unrelated adult presenting the child to healthcare services.
- Evasive or changing history.
- A trigger event such as soiling, enuresis, or minor misbehaviour by the person.
- History inconsistent with assessed development.
- A lack of parental or carer concern.
- A lack of appropriate supervision of a vulnerable person (may indicate neglect).
- Failure to engage with healthcare appointments or health promotion programmes (may indicate neglect).
- Consider the possibility of non-accidental injury if on examination:
- The history given is incompatible with examination findings.
- There are no splash marks in scald injuries (a fall into the bath will usually produce splash marks).
- There are signs of restraint on upper limbs.
- There is sparing of the flexion creases (suggests the child was in the fetal position when burnt).
- There is central sparing of the buttocks (the 'doughnut sign'), may be found in submersion injuries if a person has been forcibly held down.
- There are associated unrelated injuries (such as bruises of various ages).
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |