

Trauma
This was previously featured in an exam
A 32 year old man is brought to the Emergency Department by paramedics following a road traffic collision. He was the unrestrained front seat passenger and has "bullseyed" the windscreen. On examination you note significant bruising across the chest. His observations are recorded as:
- Heart rate: 112 beats per minute
- Blood pressure: 135/78 mmHg
- Respiratory rate: 20 breaths per minute
- GCS: Eyes 4, Voice 4, Motor 6
Whilst waiting for a trauma CT scan there is a change in his clinical condition. His observations are now:
- Heart rate: 52 beats per minute
- Blood pressure: 165/70 mmHg
- Respiratory rate: 12 breaths per minute
- GCS: Eyes 2, Voice 2, Motor 5
What is the most likely cause for the change in the patient's condition?
Answer:
- Signs of raised ICP include:
- Headache
- Early changes in mental state e.g. lethargy, irritability, agitation
- Vomiting
- Pupillary changes e.g. unequal, dilated or poorly responsive pupils
- Fundoscopy changes e.g. papilloedema
- Abnormal 'doll's eye' movements
- Focal neurological deficit e.g. CN III palsy, contralateral hemiparesis, abnormal posturing
- Cushing's triad (hypertension, bradycardia, irregular respirations)
- Late changes in mental state e.g. loss of consciousness
Head Injury: Anatomy and Pathophysiology
Trauma
Last Updated: 16th July 2025
Scalp
- Because of the scalp's generous blood supply, scalp lacerations can result in major blood loss, haemorrhagic shock and even death.
Skull
- The base of the skull is irregular and its surface can contribute to injury as the brain moves within the skull during the acceleration and deceleration that occurs in a traumatic event.
- The anterior fossa houses the frontal lobes, the middle fossa houses the temporal lobes and the posterior fossa contains the lower brainstem and cerebellum.
Meninges
The meninges cover the brain and consist of three layers: the dura mater, arachnoid mater and pia mater.
- Dura mater
- The dura mater is a tough fibrous membrane that adheres firmly to the internal surface of the skull.
- At specific sites, the dura splits into two “leaves” that enclose the large venous sinuses, which provide the major venous drainage from the brain. The midline superior sagittal sinus drains into the bilateral transverse and sigmoid sinuses, which are usually larger on the right side. Laceration of these venous sinuses can result in massive haemorrhage.
- Meningeal arteries lie between the dura and the internal surface of the skull in the epidural space. Overlying skull fractures can lacerate these arteries and cause an epidural haematoma. The most commonly injured meningeal vessel is the middle meningeal artery, which is located over the temporal fossa. An expanding haematoma from arterial injury in this location can lead to rapid deterioration and death.
- Epidural haematomas can also result from injury to the dural sinuses and from skull fractures, which tend to expand slowly and put less pressure on the underlying brain. However, most epidural haematomas constitute life-threatening emergencies that must be evaluated by a neurosurgeon as soon as possible.
- Arachnoid mater
- Beneath the dura is a second meningeal layer: the thin, transparent arachnoid mater. Because the dura is not attached to the underlying arachnoid membrane, a potential space between these layers exists (the subdural space), into which haemorrhage can occur. In brain injury, bridging veins that travel from the surface of the brain to the venous sinuses within the dura may tear, leading to the formation of a subdural haematoma.
- Pia mater
- The third layer, the pia mater, is firmly attached to the surface of the brain. Cerebrospinal fluid (CSF) fills the space between the watertight arachnoid mater and the pia mater (the subarachnoid space), cushioning the brain and spinal cord. Haemorrhage into this fluid-filled space (subarachnoid haemorrhage) frequently accompanies brain contusion and injuries to major blood vessels at the base of the brain.
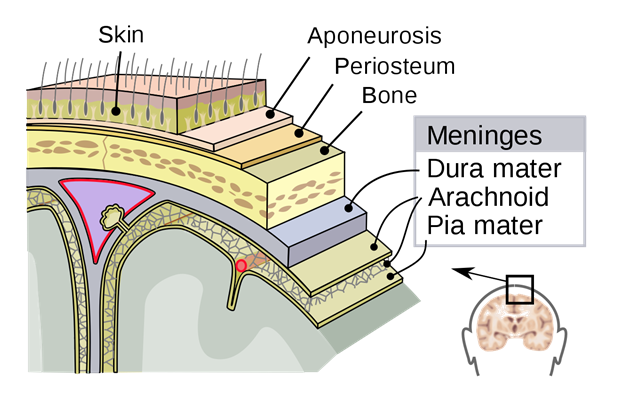
Layers of the Scalp. (Image by SVG by Mysid, original by SEER Development Team, Jmarchn [CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)])
Brain
The brain consists of the cerebrum, brainstem, and cerebellum.
- Cerebrum
- The cerebrum is composed of the right and left hemispheres, which are separated by the falx cerebri.
- The left hemisphere contains the language centers in virtually all right-handed people and in more than 85% of left-handed people.
- The frontal lobe controls executive function, emotions, motor function, and, on the dominant side, expression of speech (motor speech areas).
- The parietal lobe directs sensory function and spatial orientation, the temporal lobe regulates certain memory functions, and the occipital lobe is responsible for vision.
- Brainstem
- The brainstem is composed of the midbrain, pons, and medulla.
- The midbrain and upper pons contain the reticular activating system, which is responsible for the state of alertness.
- Vital cardiorespiratory centers reside in the medulla, which extends downward to connect with the spinal cord.
- Even small lesions in the brainstem can be associated with severe neurological deficits.
- Cerebellum
- The cerebellum, responsible mainly for coordination and balance, projects posteriorly in the posterior fossa and connects to the spinal cord, brainstem, and cerebral hemispheres.
Ventricular system
- The ventricles are a system of CSF-filled spaces and aqueducts within the brain. CSF is constantly produced within the ventricles and absorbed over the surface of the brain. The presence of blood in the CSF can impair its reabsorption, resulting in increased intracranial pressure. Oedema and mass lesions (e.g. haematomas) can cause effacement or shifting of the normally symmetric ventricles, which can readily be identified on brain CT scans.
Intracranial compartments
- Tough meningeal partitions separate the brain into regions. The tentorium cerebelli divides the intracranial cavity into the supratentorial and infratentorial compartments. The midbrain passes through an opening called the tentorial hiatus or notch.
- Uncal herniation
- The part of the brain that usually herniates through the tentorial notch is the medial part of the temporal lobe, known as the uncus.
- The oculomotor nerve (cranial nerve III) runs along the edge of the tentorium and may become compressed against it during temporal lobe herniation. Parasympathetic fibers that constrict the pupils lie on the surface of the third cranial nerve; compression of these superficial fibers during herniation causes pupillary dilation due to unopposed sympathetic activity, often referred to as a “blown” pupil.
- Uncal herniation also causes compression of the corticospinal (pyramidal) tract in the midbrain. The motor tract crosses to the opposite side at the foramen magnum, so compression at the level of the midbrain results in weakness of the opposite side of the body (contralateral hemiparesis).
- Therefore ipsilateral pupillary dilation associated with contralateral hemiparesis is the classic sign of uncal herniation. Rarely, the mass lesion pushes the opposite side of the midbrain against the tentorial edge, resulting in hemiparesis and a dilated pupil on the same side as the haematoma.
- Central herniation
- Central herniation (coning) is a late/severe sequela of supratentorial mass effect and involves descent of the diencephalon and midbrain.
- The clinical syndrome of central herniation classically manifests as a rostral to caudal progression of deficits attributed to brainstem dysfunction, including cranial nerve III (oculomotor nerve) palsy, diminished level of consciousness, decerebrate or decorticate posturing, rigidity or paralysis, abnormal respiratory pattern, and eventually death.
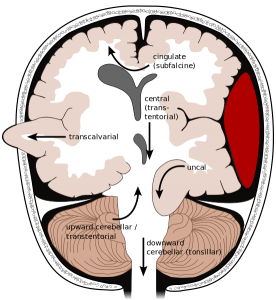
Brain Herniation Types. (Image by Brain_herniation_types.svg: User:Delldot derivative work: RupertMillard (Brain_herniation_types.svg) [CC BY-SA 3.0 , via Wikimedia Commons)
Raised intracranial pressure
- Elevation of intracranial pressure (ICP) can reduce cerebral perfusion and cause or exacerbate ischaemia.
- The cranial cavity has a fixed volume because the cranium is a rigid, non-expansive container. When the normal intracranial volume is exceeded, ICP rises.
- Venous blood and CSF can be compressed out of the container, providing a degree of pressure buffering. Thus, very early after injury, a mass such as a blood clot can enlarge while the ICP remains normal. However, once the limit of displacement of CSF and intravascular blood has been reached, ICP rapidly increases.
- The normal ICP for patients in the resting state is approximately 10 mm Hg. Pressures greater than 22 mmHg, particularly if sustained and refractory to treatment, are associated with poor outcomes.
- Signs of raised ICP include:
- Headache
- Early changes in mental state e.g. lethargy, irritability, agitation
- Vomiting
- Pupillary changes e.g. unequal, dilated or poorly responsive pupils
- Fundoscopy changes e.g. papilloedema
- Abnormal 'doll's eye' movements
- Focal neurological deficit e.g. CN III palsy, contralateral hemiparesis, abnormal posturing
- Cushing's triad (hypertension, bradycardia, irregular respirations)
- Late changes in mental state e.g. loss of consciousness
Decreased cerebral blood flow
- Traumatic brain injury (TBI) that is severe enough to cause coma can markedly reduce cerebral blood flow (CBF) during the first few hours after injury. CBF usually increases over the next 2 to 3 days, but for patients who remain comatose, it remains below normal for days or weeks after injury.
- There is increasing evidence that low levels of CBF do not meet the metabolic demands of the brain early after injury. Regional, even global, cerebral ischaemia is common after severe head injury for both known and undetermined reasons.
- The precapillary cerebral vasculature typically can reflexively constrict or dilate in response to changes in mean arterial blood pressure (MAP). For clinical purposes, cerebral perfusion pressure (CPP) is defined as mean arterial blood pressure minus intracranial pressure (CPP = MAP – ICP). A MAP of 50 to 150 mm Hg is “autoregulated” to maintain a constant CBF (pressure autoregulation).
- Severe TBI can disrupt pressure autoregulation to the point that the brain cannot adequately compensate for changes in CPP. In this situation, if the MAP is too low, ischaemia and infarction result. If the MAP is too high, marked brain swelling occurs with elevated ICP.
- Cerebral blood vessels also constrict or dilate in response to changes in the partial pressure of oxygen (PaO2) and the partial pressure of carbon dioxide (PaCO2) in the blood (chemical regulation). Therefore, secondary injury can occur from hypotension, hypoxia, hypercapnia, and iatrogenic hypocapnia.
- Every effort should be made to enhance cerebral perfusion and blood flow by reducing elevated ICP, maintaining normal intravascular volume and MAP, and restoring normal oxygenation and ventilation. Haematomas and other lesions that increase intracranial volume should be evacuated early.
- Maintaining a normal CPP may help improve CBF; however, CPP does not equate with or ensure adequate CBF. Once compensatory mechanisms are exhausted and ICP increases exponentially, brain perfusion is compromised.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |