
Questions Answered: 300
Final Score 76%
Questions
- Q1. X Incorrect
- Q2. X Incorrect
- Q3. ✓ Correct
- Q4. ✓ Correct
- Q5. ✓ Correct
- Q6. X Incorrect
- Q7. ✓ Correct
- Q8. ✓ Correct
- Q9. ✓ Correct
- Q10. ✓ Correct
- Q11. ✓ Correct
- Q12. X Incorrect
- Q13. ✓ Correct
- Q14. X Incorrect
- Q15. ✓ Correct
- Q16. ✓ Correct
- Q17. ✓ Correct
- Q18. ✓ Correct
- Q19. ✓ Correct
- Q20. ✓ Correct
- Q21. ✓ Correct
- Q22. ✓ Correct
- Q23. ✓ Correct
- Q24. ✓ Correct
- Q25. ✓ Correct
- Q26. X Incorrect
- Q27. ✓ Correct
- Q28. ✓ Correct
- Q29. ✓ Correct
- Q30. ✓ Correct
- Q31. ✓ Correct
- Q32. ✓ Correct
- Q33. ✓ Correct
- Q34. ✓ Correct
- Q35. ✓ Correct
- Q36. ✓ Correct
- Q37. X Incorrect
- Q38. ✓ Correct
- Q39. X Incorrect
- Q40. ✓ Correct
- Q41. X Incorrect
- Q42. ✓ Correct
- Q43. ✓ Correct
- Q44. X Incorrect
- Q45. X Incorrect
- Q46. X Incorrect
- Q47. X Incorrect
- Q48. ✓ Correct
- Q49. X Incorrect
- Q50. ✓ Correct
- Q51. ✓ Correct
- Q52. ✓ Correct
- Q53. ✓ Correct
- Q54. X Incorrect
- Q55. X Incorrect
- Q56. X Incorrect
- Q57. X Incorrect
- Q58. ✓ Correct
- Q59. ✓ Correct
- Q60. ✓ Correct
- Q61. ✓ Correct
- Q62. ✓ Correct
- Q63. X Incorrect
- Q64. ✓ Correct
- Q65. ✓ Correct
- Q66. X Incorrect
- Q67. ✓ Correct
- Q68. ✓ Correct
- Q69. ✓ Correct
- Q70. ✓ Correct
- Q71. ✓ Correct
- Q72. ✓ Correct
- Q73. ✓ Correct
- Q74. ✓ Correct
- Q75. X Incorrect
- Q76. ✓ Correct
- Q77. ✓ Correct
- Q78. ✓ Correct
- Q79. ✓ Correct
- Q80. X Incorrect
- Q81. ✓ Correct
- Q82. ✓ Correct
- Q83. ✓ Correct
- Q84. ✓ Correct
- Q85. X Incorrect
- Q86. ✓ Correct
- Q87. ✓ Correct
- Q88. ✓ Correct
- Q89. ✓ Correct
- Q90. ✓ Correct
- Q91. ✓ Correct
- Q92. ✓ Correct
- Q93. ✓ Correct
- Q94. X Incorrect
- Q95. ✓ Correct
- Q96. X Incorrect
- Q97. ✓ Correct
- Q98. X Incorrect
- Q99. X Incorrect
- Q100. ✓ Correct
- Q101. ✓ Correct
- Q102. ✓ Correct
- Q103. ✓ Correct
- Q104. ✓ Correct
- Q105. ✓ Correct
- Q106. ✓ Correct
- Q107. ✓ Correct
- Q108. ✓ Correct
- Q109. ✓ Correct
- Q110. X Incorrect
- Q111. ✓ Correct
- Q112. ✓ Correct
- Q113. ✓ Correct
- Q114. X Incorrect
- Q115. X Incorrect
- Q116. ✓ Correct
- Q117. X Incorrect
- Q118. X Incorrect
- Q119. ✓ Correct
- Q120. ✓ Correct
- Q121. ✓ Correct
- Q122. ✓ Correct
- Q123. X Incorrect
- Q124. ✓ Correct
- Q125. ✓ Correct
- Q126. X Incorrect
- Q127. X Incorrect
- Q128. ✓ Correct
- Q129. ✓ Correct
- Q130. X Incorrect
- Q131. ✓ Correct
- Q132. ✓ Correct
- Q133. ✓ Correct
- Q134. ✓ Correct
- Q135. X Incorrect
- Q136. ✓ Correct
- Q137. ✓ Correct
- Q138. ✓ Correct
- Q139. ✓ Correct
- Q140. ✓ Correct
- Q141. ✓ Correct
- Q142. ✓ Correct
- Q143. ✓ Correct
- Q144. ✓ Correct
- Q145. ✓ Correct
- Q146. ✓ Correct
- Q147. ✓ Correct
- Q148. ✓ Correct
- Q149. ✓ Correct
- Q150. ✓ Correct
- Q151. X Incorrect
- Q152. ✓ Correct
- Q153. X Incorrect
- Q154. ✓ Correct
- Q155. ✓ Correct
- Q156. ✓ Correct
- Q157. ✓ Correct
- Q158. ✓ Correct
- Q159. ✓ Correct
- Q160. ✓ Correct
- Q161. ✓ Correct
- Q162. ✓ Correct
- Q163. ✓ Correct
- Q164. ✓ Correct
- Q165. X Incorrect
- Q166. ✓ Correct
- Q167. ✓ Correct
- Q168. ✓ Correct
- Q169. ✓ Correct
- Q170. ✓ Correct
- Q171. ✓ Correct
- Q172. ✓ Correct
- Q173. ✓ Correct
- Q174. ✓ Correct
- Q175. X Incorrect
- Q176. X Incorrect
- Q177. ✓ Correct
- Q178. ✓ Correct
- Q179. ✓ Correct
- Q180. X Incorrect
- Q181. ✓ Correct
- Q182. ✓ Correct
- Q183. ✓ Correct
- Q184. X Incorrect
- Q185. ✓ Correct
- Q186. ✓ Correct
- Q187. ✓ Correct
- Q188. X Incorrect
- Q189. X Incorrect
- Q190. ✓ Correct
- Q191. ✓ Correct
- Q192. ✓ Correct
- Q193. ✓ Correct
- Q194. X Incorrect
- Q195. ✓ Correct
- Q196. ✓ Correct
- Q197. ✓ Correct
- Q198. ✓ Correct
- Q199. ✓ Correct
- Q200. ✓ Correct
- Q201. X Incorrect
- Q202. X Incorrect
- Q203. ✓ Correct
- Q204. ✓ Correct
- Q205. ✓ Correct
- Q206. ✓ Correct
- Q207. ✓ Correct
- Q208. ✓ Correct
- Q209. X Incorrect
- Q210. ✓ Correct
- Q211. ✓ Correct
- Q212. X Incorrect
- Q213. ✓ Correct
- Q214. ✓ Correct
- Q215. ✓ Correct
- Q216. ✓ Correct
- Q217. X Incorrect
- Q218. ✓ Correct
- Q219. ✓ Correct
- Q220. X Incorrect
- Q221. ✓ Correct
- Q222. ✓ Correct
- Q223. X Incorrect
- Q224. ✓ Correct
- Q225. X Incorrect
- Q226. ✓ Correct
- Q227. X Incorrect
- Q228. ✓ Correct
- Q229. ✓ Correct
- Q230. ✓ Correct
- Q231. ✓ Correct
- Q232. ✓ Correct
- Q233. ✓ Correct
- Q234. ✓ Correct
- Q235. ✓ Correct
- Q236. ✓ Correct
- Q237. ✓ Correct
- Q238. X Incorrect
- Q239. ✓ Correct
- Q240. X Incorrect
- Q241. ✓ Correct
- Q242. X Incorrect
- Q243. ✓ Correct
- Q244. X Incorrect
- Q245. ✓ Correct
- Q246. ✓ Correct
- Q247. ✓ Correct
- Q248. ✓ Correct
- Q249. ✓ Correct
- Q250. ✓ Correct
- Q251. ✓ Correct
- Q252. X Incorrect
- Q253. ✓ Correct
- Q254. X Incorrect
- Q255. X Incorrect
- Q256. ✓ Correct
- Q257. ✓ Correct
- Q258. ✓ Correct
- Q259. ✓ Correct
- Q260. ✓ Correct
- Q261. ✓ Correct
- Q262. ✓ Correct
- Q263. ✓ Correct
- Q264. ✓ Correct
- Q265. X Incorrect
- Q266. X Incorrect
- Q267. ✓ Correct
- Q268. ✓ Correct
- Q269. ✓ Correct
- Q270. ✓ Correct
- Q271. ✓ Correct
- Q272. ✓ Correct
- Q273. ✓ Correct
- Q274. ✓ Correct
- Q275. X Incorrect
- Q276. X Incorrect
- Q277. ✓ Correct
- Q278. ✓ Correct
- Q279. ✓ Correct
- Q280. ✓ Correct
- Q281. ✓ Correct
- Q282. ✓ Correct
- Q283. ✓ Correct
- Q284. ✓ Correct
- Q285. ✓ Correct
- Q286. ✓ Correct
- Q287. ✓ Correct
- Q288. ✓ Correct
- Q289. ✓ Correct
- Q290. ✓ Correct
- Q291. ✓ Correct
- Q292. ✓ Correct
- Q293. ✓ Correct
- Q294. ✓ Correct
- Q295. ✓ Correct
- Q296. ✓ Correct
- Q297. X Incorrect
- Q298. X Incorrect
- Q299. X Incorrect
- Q300. X Incorrect

Maxillofacial & Dental
An 18 year old rugby player is brought to the Emergency Department by his teammates. He was punched to the face during a game. On examination you note orbital emphysema and paraesthesia in the malar region. Which nerve is most likely injured?
Answer:
The infraorbital nerve can be injured in an orbital floor fracture and cause numbness to the malar region.Orbital Blowout Fracture
Maxillofacial & Dental
Last Updated: 14th December 2023
In an orbital blowout fracture, the pressure from a direct blow involving the relatively tough globe is transmitted downwards, fracturing the floor of the orbit, and often results in herniation of intraocular contents into the maxillary sinus. This type of fracture typically occurs due to a direct blow to the central orbit e.g. from a fist, ball, elbow, dashboard or car seat.
Clinical anatomy
The bony orbit is composed of thickened orbital rims (margins) but relatively thin inner walls. The zygoma and maxilla form the greater part of the medial, inferior and lateral orbital margins as well as almost all of the orbital floor.
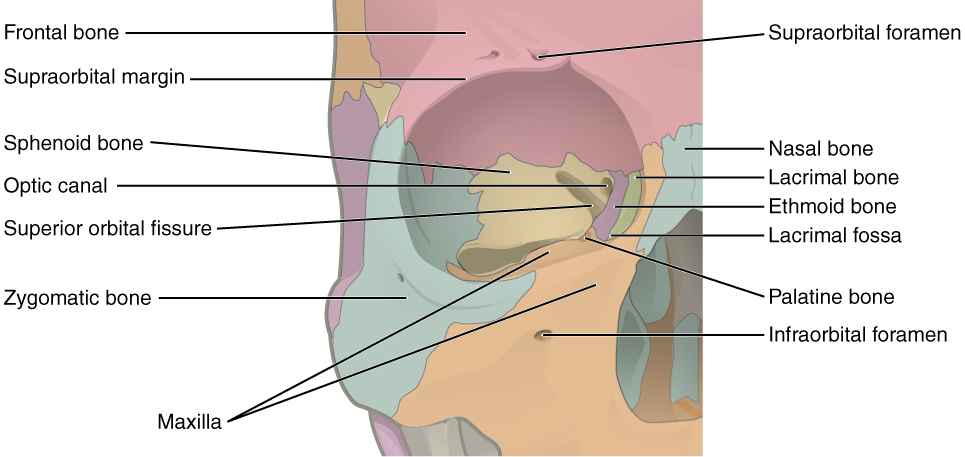
Bony Orbit. (Image by OpenStax College [CC BY 3.0 , via Wikimedia Commons)
Clinical features
- Enophthalmos (due to increased orbital volume)
- Diplopia/ophthalmoplegia, particularly upward gaze (due to trapping of the herniated inferior rectus muscle)
- Orbital emphysema (fracture into adjacent paranasal sinus, usually the maxillary)
- Malar region numbness (injury to infraorbital nerve)
- Subconjunctival haemorrhage – if a clear posterior border cannot be seen , it is likely blood has tracked round the eye from a fracture of the orbital wall
Diagnosis
The diagnosis of an orbital blowout fracture may be made on routine facial x-rays (e.g. a 'teardrop' sign caused by soft tissue herniating through roof of maxillary sinus) but CT scan remains the gold standard if this injury is suspected or identified.
Relatively recently, focused ocular ultrasound (FOUS) has been evaluated in the ED and found to be highly accurate in both diagnosing and excluding both orbital and ocular trauma.
Management
Clinical suspicion of an orbital blowout fracture (e.g. diplopia or reduced eye movements) merits urgent referral to a maxillofacial surgeon and/or an ophthalmologist.
Although plain x-ray may reinforce suspicion, facial CT scan will be needed to visualise the fracture in detail and plan surgical repair.
There is no evidence to support routine antibiotic prophylaxis in orbital floor fracture (despite risk of orbital cellulitis) and local guidance should be followed.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |
Are you sure you wish to end this session?