

Surgical Emergencies
This was previously featured in an exam
An 18 month old is brought to ED by her mum with crying episodes occurring over the past 12 hours. During these episodes she is crying in pain, holding her abdomen and drawing up her legs to her abdomen whilst lying down. Her mum also describes mucus and blood mixed in with stool seen in her nappy. What is the most likely diagnosis?
Answer:
Most intussusceptions are seen in children between 3 months and 3 years, most commonly in infants under 1 year of age. Boys are more commonly affected than girls. They may present with paroxysms of colicky abdominal pain and crying (during the attack the child becomes pale, distressed and draws up the legs). The child may appear well between paroxysms initially. There is early vomiting. So-called redcurrant jelly stools may be passed (which consist of mucus and blood). Abdominal examination may reveal a distended abdomen, a palpable sausage-shaped mass (often in the RUQ) and absence of bowel in the right lower quadrant (Dance's sign).Intussusception
Surgical Emergencies
Last Updated: 14th December 2023
Clinical anatomy
Intussusception is the telescoping of one portion of the intestine (the intussusceptum) into the lumen of the intestine immediately distal to it (the intussuscipiens). The mesentery is dragged alongside the proximal bowel wall into the distal lumen resulting in obstruction of venous return. Oedema, mucosal bleeding, and increased pressure result. If arterial flow becomes compromised, ischaemia, necrosis, and perforation can occur.
Ileocolonic intussusception (prolapse of the terminal ileum into the proximal colon) is the most common anatomical location for intussusception to occur, followed by ileoileal and colocolonic.
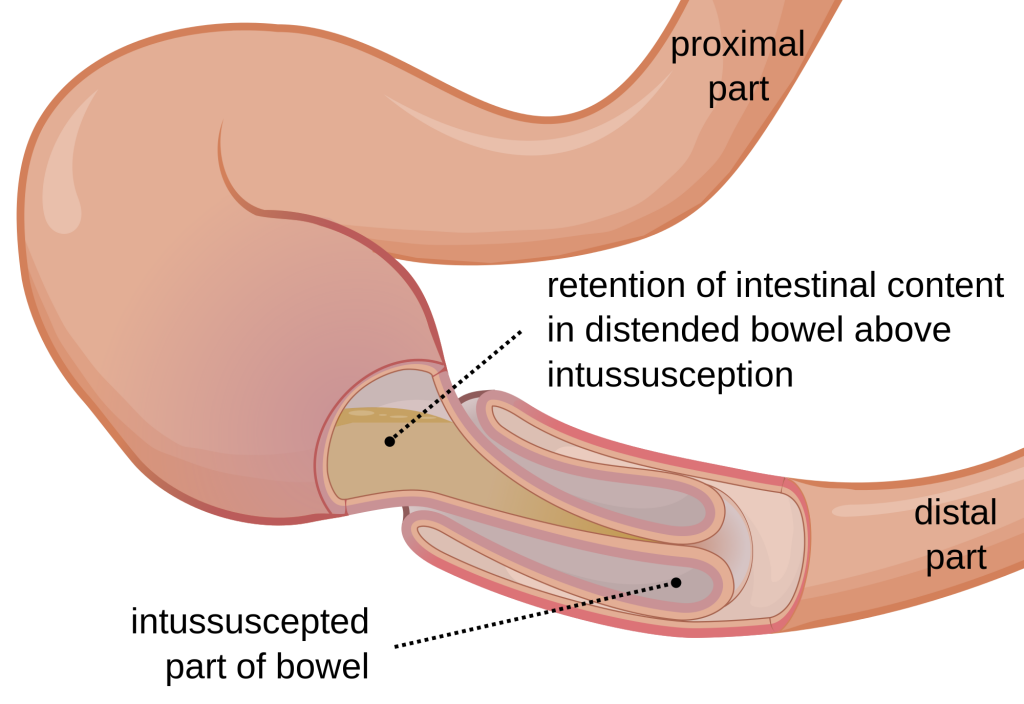
Intussusception. (Image by Olek Remesz (wiki-pl: Orem, commons: Orem) (Own work) [CC BY-SA 3.0 , via Wikimedia Commons)
Causes
The aetiology of most cases of intussusception is unclear but is likely to be related to hyperplasia of Peyer's patches and lymphoid tissue in the intestinal wall resulting from antecedent viral infection. These enlarged lymph nodes may act as the lead point in idiopathic intussusception.
Intussusception in older children and adults is rare and is almost always caused by a pathological lead point. Pathological lead points are anatomical abnormalities of the intestine, such as luminal polyps, malignant tumours (including lymphoma), and benign mass lesions (e.g. lipomata, Meckel's diverticulum, Henoch-Schonlein purpura, and enteric duplication cysts.
Clinical features
Most intussusceptions are seen in children between 3 months and 3 years, most commonly in infants under 1 year of age. Boys are more commonly affected than girls. They may present with paroxysms of colicky abdominal pain and crying (during the attack the child becomes pale, distressed and draws up the legs). The child may appear well between paroxysms initially. There is early vomiting. So-called redcurrant jelly stools may be passed (which consist of mucus and blood). Abdominal examination may reveal a distended abdomen, a palpable sausage-shaped mass (often in the RUQ) and absence of bowel in the right lower quadrant (Dance's sign).
Differential diagnosis
- Appendicitis
- Gastroenteritis
- Urinary tract infection
- Pyloric stenosis
Investigations
- The target sign (variants according to appearance or imaging modality include bull’s eye sign, doughnut sign, crescent-in-doughnut sign, and multiple concentric ring sign) is a single hypoechoic ring with a hyperechoic centre, indicating that one portion of the bowel has been drawn within the lumen of an adjacent portion.
- Abdominal x-ray:
- Performed as initial investigation if perforation or obstruction is suspected.
- Plain abdominal films may be normal, or may show the typical target sign. Other suggestive signs include the presence of a soft-tissue mass, an empty right lower quadrant, air in a dislocated appendix, free intra-abdominal air and signs of a small-bowel obstruction.
- Ultrasound:
- If the patient is clinically stable and perforation is not suspected, ultrasonography should be the initial diagnostic test for intussusception. Ultrasound has a reported diagnostic accuracy of up to 100%. The presence of a 3 to 5 cm mass just deep to the right-sided abdominal wall with the characteristic doughnut sonographical appearance is diagnostic of intussusception.
- Contrast enema:
- A contrast enema (air or contrast reagent) can be performed to diagnose intussusception but is contraindicated in the presence of free intra-abdominal air. Liquid or air enema remain the most specific and sensitive diagnostic tests and can localise the extent of the process.
- CT abdomen:
- Normally not indicated for the evaluation of intussusception. May be used to assess for the presence and identification of a pathological lead point.
Management
Stable patients with a high clinical suspicion and/or radiographic evidence of intussusception and no evidence of bowel perforation should be treated with nonoperative reduction using hydrostatic or pneumatic pressure by contrast enema (air or liquid contrast).
Surgical treatment is indicated as a primary intervention for patients with suspected intussusception who are acutely ill or have evidence of perforation, peritonitis or shock.
Complications
- Ischaemia, infarction and necrosis
- Obstruction
- Perforation
- Peritonitis
- Sepsis
- Haemorrhage
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |