

Respiratory
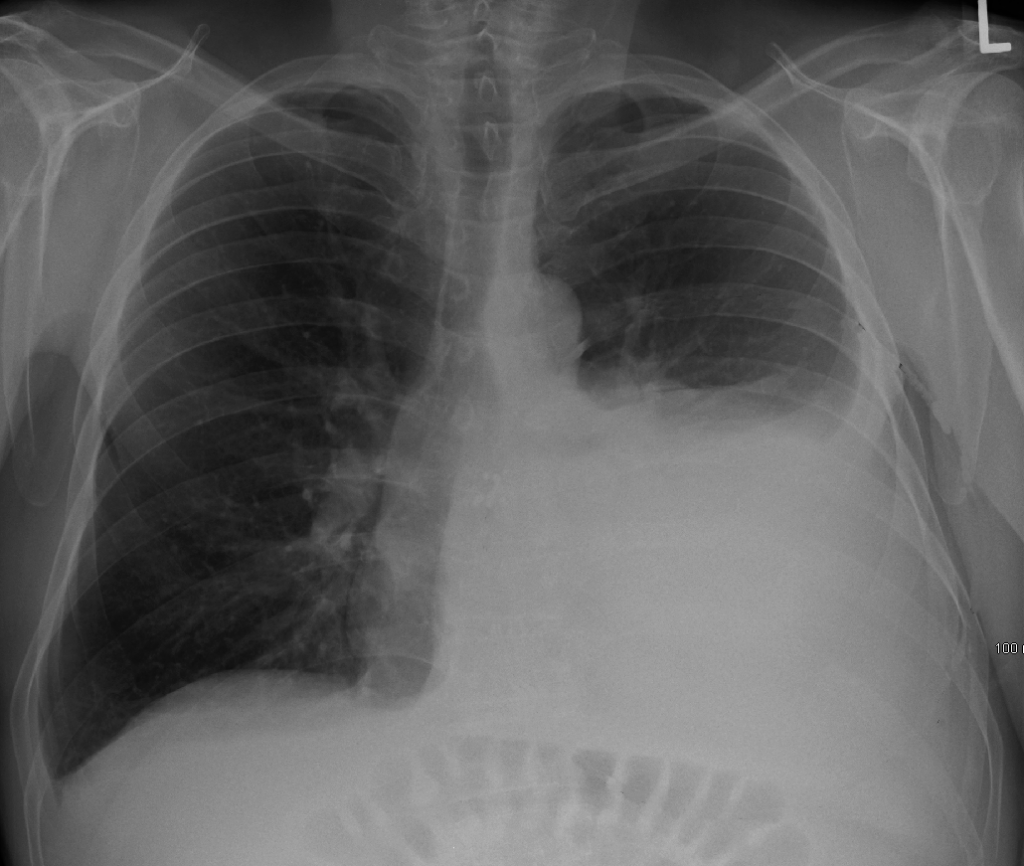
A 65 year old lifelong smoker presents to the Emergency Department with a 3 week history of progressive breathlessness on exertion. What is the single most likely diagnosis?
Answer:
The chest x-ray shows a large left sided pleural effusion.Pleural Effusion
Oncology & Palliative Care / Respiratory
Last Updated: 6th September 2022
Pleural fluid volume is maintained by the balance of pulmonary capillary hydrostatic and oncotic pressure, lymphatic drainage and the integrity of the pleural and capillary membranes. Pleural effusion occurs when fluid collects in the pleural space between the parietal and visceral pleura. If the fluid becomes infected an empyema results.
Pathophysiology
- Transudates are associated with increased systemic or pulmonary capillary hydrostatic pressure or decreased colloid osmotic pressure. The pleural membranes are intact and the permeability of pleural capillaries to proteins is normal.
- Exudates are associated with altered permeability of pleural membranes, increased capillary wall permeability to proteins or vascular disruption. They can also be associated with reduced or obstructed lymphatic drainage from the pleural space.
Causes
- Transudate (protein < 25 g/L)
- Congestive heart failure
- Liver failure/cirrhosis
- Hypoalbuminaemia
- Peritoneal dialysis
- Hypothyroidism
- Renal failure/nephrotic syndrome
- Mitral stenosis
- Pulmonary embolism (80% exudates, 20% transudates)
- Exudate (protein > 35 g/L)
- Pneumonia
- Malignancy (most commonly, lung, breast, lymphoma, tumours of the GI tract)
- Tuberculosis
- Pulmonary embolism (80% exudates, 20% transudates)
- Autoimmune disease (especially rheumatoid arthritis)
- Asbestos exposure
- Pancreatitis
- Dressler’s syndrome (following acute myocardial infarction)
- Haemothorax
- Empyema
- Chylothorax
Clinical features
- Symptoms
- Pleuritic chest pain
- Dyspnoea
- Tachypnoea
- Cough
- Signs
- Respiratory distress
- Reduced chest expansion
- Tracheal deviation away from large effusion
- Decreased tactile/vocal fremitus
- Stony dullness on percussion
- Reduced breath sounds
Investigations
- Chest x-ray
- The most common first line imaging is a chest radiograph showing blunting of the costophrenic angle
- About 200 ml of fluid needed to be visible on a PA view and about 50 ml on a lateral view
- Ultrasound
- Point of care ultrasound is being increasingly used in Emergency Departments to help guide diagnosis and treatment. It can provide a rapid diagnosis at the bedside and is particularly helpful in those patients who are acutely unwell
- Diagnostic pleural aspiration with ultrasound guidance
- Send for protein, LDH, cytology, fluid pH, glucose, Gram stain, culture and sensitivity
- Aspiration should not be performed for bilateral effusions in a clinical setting strongly suggestive of a transudate unless there are atypical features or they fail to respond to therapy
- Contrast enhanced CT thorax
- If fluid analysis and clinical features do not confirm the diagnosis or underlying cause
- Bloods
- ABG (if hypoxic)
- FBC & CRP (to assess inflammatory response)
- U&Es & LFTs (to look for underlying cause)
- Serum protein, LDH and glucose (for Light's criteria)
- Serum amylase (if pancreatitis suspected)
- D-dimer (if PE suspected)
- Consider invasive investigations
- LA thoracostomy or surgical VATS
- Percutaneous pleural biopsy +/- chest tube drainage if symptomatic
Pleural fluid analysis
The appearance of the pleural fluid and any odour should be recorded.
Fluid may appear serous, blood-tinged, frankly bloody or purulent. Centrifuging turbid or milky pleural fluid will distinguish between empyema and lipid effusions. If the supernatant is clear, the turbid fluid was due to cell debris and empyema is likely while, if it is still turbid, chylothorax or pseudochylothorax are likely. Grossly bloody pleural fluid is usually due to malignancy, pulmonary embolism with infarction, trauma, benign asbestos pleural effusions or post-cardiac injury syndrome. A haemothorax can be distinguished from other blood-stained effusions by performing a haematocrit on the pleural fluid. A pleural fluid haematocrit >50% of the patient’s peripheral blood haematocrit is diagnostic of a haemothorax.
Light's criteria can be used to accurately differentiate between a transudate and exudate (particularly where pleural fluid protein is between 25 – 35 g/L):
Fluid is considered exudative if one of the following criteria is present:
- Pleural fluid-to-serum protein ratio > 0.5; or
- Pleural fluid-to-serum LDH ratio > 0.6; or
- Pleural fluid LDH concentration > two thirds upper limit of normal for serum LDH.
Management
There is no national consensus on which patients should undergo diagnostic aspiration, therapeutic aspiration or drainage in the ED. The most common indication for drainage in ED is large effusion causing significant hypoxia or distress, particularly those associated with mediastinal shift. Definitive management depends on the underlying cause.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |