
Questions Answered: 300
Final Score 76%
Questions
- Q1. X Incorrect
- Q2. X Incorrect
- Q3. ✓ Correct
- Q4. ✓ Correct
- Q5. ✓ Correct
- Q6. X Incorrect
- Q7. ✓ Correct
- Q8. ✓ Correct
- Q9. ✓ Correct
- Q10. ✓ Correct
- Q11. ✓ Correct
- Q12. X Incorrect
- Q13. ✓ Correct
- Q14. X Incorrect
- Q15. ✓ Correct
- Q16. ✓ Correct
- Q17. ✓ Correct
- Q18. ✓ Correct
- Q19. ✓ Correct
- Q20. ✓ Correct
- Q21. ✓ Correct
- Q22. ✓ Correct
- Q23. ✓ Correct
- Q24. ✓ Correct
- Q25. ✓ Correct
- Q26. X Incorrect
- Q27. ✓ Correct
- Q28. ✓ Correct
- Q29. ✓ Correct
- Q30. ✓ Correct
- Q31. ✓ Correct
- Q32. ✓ Correct
- Q33. ✓ Correct
- Q34. ✓ Correct
- Q35. ✓ Correct
- Q36. ✓ Correct
- Q37. X Incorrect
- Q38. ✓ Correct
- Q39. X Incorrect
- Q40. ✓ Correct
- Q41. X Incorrect
- Q42. ✓ Correct
- Q43. ✓ Correct
- Q44. X Incorrect
- Q45. X Incorrect
- Q46. X Incorrect
- Q47. X Incorrect
- Q48. ✓ Correct
- Q49. X Incorrect
- Q50. ✓ Correct
- Q51. ✓ Correct
- Q52. ✓ Correct
- Q53. ✓ Correct
- Q54. X Incorrect
- Q55. X Incorrect
- Q56. X Incorrect
- Q57. X Incorrect
- Q58. ✓ Correct
- Q59. ✓ Correct
- Q60. ✓ Correct
- Q61. ✓ Correct
- Q62. ✓ Correct
- Q63. X Incorrect
- Q64. ✓ Correct
- Q65. ✓ Correct
- Q66. X Incorrect
- Q67. ✓ Correct
- Q68. ✓ Correct
- Q69. ✓ Correct
- Q70. ✓ Correct
- Q71. ✓ Correct
- Q72. ✓ Correct
- Q73. ✓ Correct
- Q74. ✓ Correct
- Q75. X Incorrect
- Q76. ✓ Correct
- Q77. ✓ Correct
- Q78. ✓ Correct
- Q79. ✓ Correct
- Q80. X Incorrect
- Q81. ✓ Correct
- Q82. ✓ Correct
- Q83. ✓ Correct
- Q84. ✓ Correct
- Q85. X Incorrect
- Q86. ✓ Correct
- Q87. ✓ Correct
- Q88. ✓ Correct
- Q89. ✓ Correct
- Q90. ✓ Correct
- Q91. ✓ Correct
- Q92. ✓ Correct
- Q93. ✓ Correct
- Q94. X Incorrect
- Q95. ✓ Correct
- Q96. X Incorrect
- Q97. ✓ Correct
- Q98. X Incorrect
- Q99. X Incorrect
- Q100. ✓ Correct
- Q101. ✓ Correct
- Q102. ✓ Correct
- Q103. ✓ Correct
- Q104. ✓ Correct
- Q105. ✓ Correct
- Q106. ✓ Correct
- Q107. ✓ Correct
- Q108. ✓ Correct
- Q109. ✓ Correct
- Q110. X Incorrect
- Q111. ✓ Correct
- Q112. ✓ Correct
- Q113. ✓ Correct
- Q114. X Incorrect
- Q115. X Incorrect
- Q116. ✓ Correct
- Q117. X Incorrect
- Q118. X Incorrect
- Q119. ✓ Correct
- Q120. ✓ Correct
- Q121. ✓ Correct
- Q122. ✓ Correct
- Q123. X Incorrect
- Q124. ✓ Correct
- Q125. ✓ Correct
- Q126. X Incorrect
- Q127. X Incorrect
- Q128. ✓ Correct
- Q129. ✓ Correct
- Q130. X Incorrect
- Q131. ✓ Correct
- Q132. ✓ Correct
- Q133. ✓ Correct
- Q134. ✓ Correct
- Q135. X Incorrect
- Q136. ✓ Correct
- Q137. ✓ Correct
- Q138. ✓ Correct
- Q139. ✓ Correct
- Q140. ✓ Correct
- Q141. ✓ Correct
- Q142. ✓ Correct
- Q143. ✓ Correct
- Q144. ✓ Correct
- Q145. ✓ Correct
- Q146. ✓ Correct
- Q147. ✓ Correct
- Q148. ✓ Correct
- Q149. ✓ Correct
- Q150. ✓ Correct
- Q151. X Incorrect
- Q152. ✓ Correct
- Q153. X Incorrect
- Q154. ✓ Correct
- Q155. ✓ Correct
- Q156. ✓ Correct
- Q157. ✓ Correct
- Q158. ✓ Correct
- Q159. ✓ Correct
- Q160. ✓ Correct
- Q161. ✓ Correct
- Q162. ✓ Correct
- Q163. ✓ Correct
- Q164. ✓ Correct
- Q165. X Incorrect
- Q166. ✓ Correct
- Q167. ✓ Correct
- Q168. ✓ Correct
- Q169. ✓ Correct
- Q170. ✓ Correct
- Q171. ✓ Correct
- Q172. ✓ Correct
- Q173. ✓ Correct
- Q174. ✓ Correct
- Q175. X Incorrect
- Q176. X Incorrect
- Q177. ✓ Correct
- Q178. ✓ Correct
- Q179. ✓ Correct
- Q180. X Incorrect
- Q181. ✓ Correct
- Q182. ✓ Correct
- Q183. ✓ Correct
- Q184. X Incorrect
- Q185. ✓ Correct
- Q186. ✓ Correct
- Q187. ✓ Correct
- Q188. X Incorrect
- Q189. X Incorrect
- Q190. ✓ Correct
- Q191. ✓ Correct
- Q192. ✓ Correct
- Q193. ✓ Correct
- Q194. X Incorrect
- Q195. ✓ Correct
- Q196. ✓ Correct
- Q197. ✓ Correct
- Q198. ✓ Correct
- Q199. ✓ Correct
- Q200. ✓ Correct
- Q201. X Incorrect
- Q202. X Incorrect
- Q203. ✓ Correct
- Q204. ✓ Correct
- Q205. ✓ Correct
- Q206. ✓ Correct
- Q207. ✓ Correct
- Q208. ✓ Correct
- Q209. X Incorrect
- Q210. ✓ Correct
- Q211. ✓ Correct
- Q212. X Incorrect
- Q213. ✓ Correct
- Q214. ✓ Correct
- Q215. ✓ Correct
- Q216. ✓ Correct
- Q217. X Incorrect
- Q218. ✓ Correct
- Q219. ✓ Correct
- Q220. X Incorrect
- Q221. ✓ Correct
- Q222. ✓ Correct
- Q223. X Incorrect
- Q224. ✓ Correct
- Q225. X Incorrect
- Q226. ✓ Correct
- Q227. X Incorrect
- Q228. ✓ Correct
- Q229. ✓ Correct
- Q230. ✓ Correct
- Q231. ✓ Correct
- Q232. ✓ Correct
- Q233. ✓ Correct
- Q234. ✓ Correct
- Q235. ✓ Correct
- Q236. ✓ Correct
- Q237. ✓ Correct
- Q238. X Incorrect
- Q239. ✓ Correct
- Q240. X Incorrect
- Q241. ✓ Correct
- Q242. X Incorrect
- Q243. ✓ Correct
- Q244. X Incorrect
- Q245. ✓ Correct
- Q246. ✓ Correct
- Q247. ✓ Correct
- Q248. ✓ Correct
- Q249. ✓ Correct
- Q250. ✓ Correct
- Q251. ✓ Correct
- Q252. X Incorrect
- Q253. ✓ Correct
- Q254. X Incorrect
- Q255. X Incorrect
- Q256. ✓ Correct
- Q257. ✓ Correct
- Q258. ✓ Correct
- Q259. ✓ Correct
- Q260. ✓ Correct
- Q261. ✓ Correct
- Q262. ✓ Correct
- Q263. ✓ Correct
- Q264. ✓ Correct
- Q265. X Incorrect
- Q266. X Incorrect
- Q267. ✓ Correct
- Q268. ✓ Correct
- Q269. ✓ Correct
- Q270. ✓ Correct
- Q271. ✓ Correct
- Q272. ✓ Correct
- Q273. ✓ Correct
- Q274. ✓ Correct
- Q275. X Incorrect
- Q276. X Incorrect
- Q277. ✓ Correct
- Q278. ✓ Correct
- Q279. ✓ Correct
- Q280. ✓ Correct
- Q281. ✓ Correct
- Q282. ✓ Correct
- Q283. ✓ Correct
- Q284. ✓ Correct
- Q285. ✓ Correct
- Q286. ✓ Correct
- Q287. ✓ Correct
- Q288. ✓ Correct
- Q289. ✓ Correct
- Q290. ✓ Correct
- Q291. ✓ Correct
- Q292. ✓ Correct
- Q293. ✓ Correct
- Q294. ✓ Correct
- Q295. ✓ Correct
- Q296. ✓ Correct
- Q297. X Incorrect
- Q298. X Incorrect
- Q299. X Incorrect
- Q300. X Incorrect

Maxillofacial & Dental
A 19 year old man presents to the Emergency Department with a history of "jaw pain" and trismus after yawning. You suspect an anterior temporomandibular joint (TMJ) dislocation. Which of the following is a risk factor for TMJ dislocation?
Answer:
Connective tissue disorders, such as Marfan's and Ehlers-Danlos syndrome, increase likelihood of TMJ dislocation.Temporomandibular Joint Dislocation
Maxillofacial & Dental
Last Updated: 14th December 2023
Dislocation of the temporomandibular joint (TMJ) is an infrequent presentation to the ED. Approximately 90% of all cases are bilateral and anterior, and the most common cause found in one survey was excessive mouth opening whilst yawning.
Clinical anatomy
The mandibular condyle of the mandible articulates with the mandibular fossa of the temporal bone forming the temporomandibular joints. The temporomandibular joint is split into two sections by an articular disc, a fibrocartilaginous structure that enables a greater range of movement of the joint.
Temporomandibular dislocations may be unilateral or bilateral and occur in anterior, posterior, lateral and superior positions. The anterior is by far the most common, the others all being associated with a fracture of either the mandible or base of the skull.
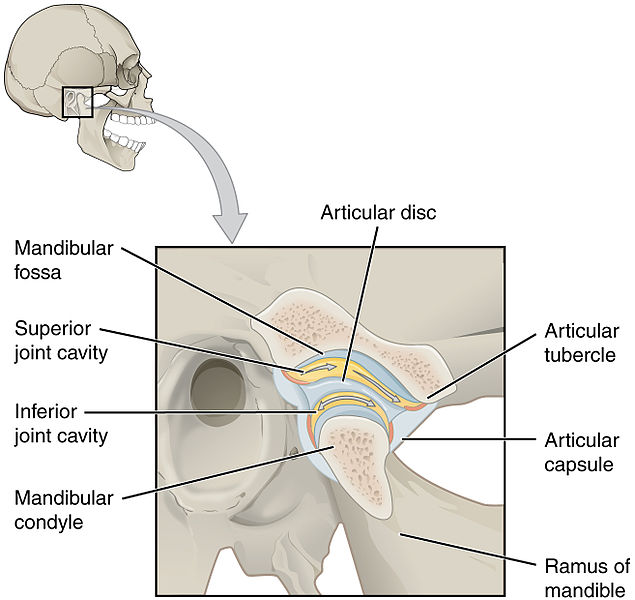
Temporomandibular Joint. (Image by OpenStax College [CC BY 3.0 , via Wikimedia Commons)
Mechanism of injury
Anterior dislocation may be traumatic or atraumatic; in trauma it is normally caused by direct downward force to a partially opened mouth.
In predisposed patients with shallow mandibular fossae or underdeveloped mandibular condyles, certain repeated activities may initially sublux, then dislocate, the mandible. The most common mechanism relates to excessive opening of the mouth when:
- Yawning
- Laughing
- Shouting
- Eating
- During dental work
Connective tissue disorders, such as Marfan's and Ehlers-Danlos syndrome, increase likelihood of dislocation. Once the mandible has dislocated anteriorly, spasm of the masseter and pterygoid muscles occurs which further traps the dislocated condyle.
Management
- The standard intraoral technique for reduction of the anteriorly dislocated TMJ is designed to push the mandible inferiorly and posteriorly back into the mandibular fossa. This can be done from either an anterior or posterior approach.
- When manipulating the mandible with an intraoral technique it is important to wear strong gloves and position the thumbs behind the last molars to ensure protection against a human bite occurring when the mouth snaps closed due to muscle spasm. A bite block may also be used.
- To facilitate reduction, it is common practice to administer an opioid analgesic and sedative agent such as midazolam, although reduction using propofol bolus has also been described.
- If the standard technique fails, other techniques have also been described involving intra-articular injection of local anaesthetic, extraoral techniques and a wrist pivot method. On rare occasions, general anaesthesia may be required using either a closed or open reduction.
- Dislocations to the posterior, medial or lateral side are usually associated with a fracture of the mandible and should be referred to a maxillofacial surgeon for reduction.
- Once the mandible has been relocated, the patient must have a repeat x-ray to confirm position and to exclude a fracture occurring on reduction.
Discharge advice
Discharge advice must include:
- Eating a soft diet in the first few days to minimise stress on the TMJ
- Avoiding wide mouth opening for the next 2 weeks and supporting the mouth with the hand if yawning or laughing
An encircling bandage (Barton bandage) to support the mandible is usually unnecessary unless the patient is unable to understand or comply with discharge advice.
All patients should be followed up by a maxillofacial specialist.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |
Are you sure you wish to end this session?