

Cardiology
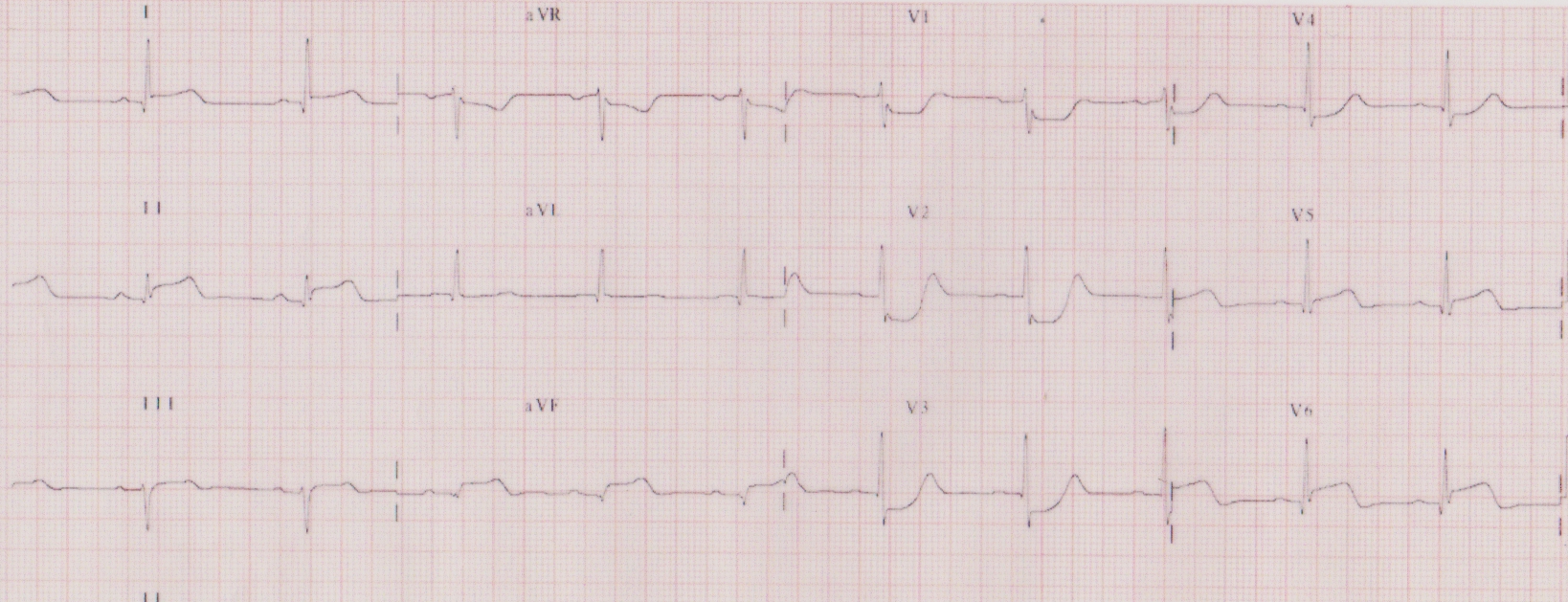 A 47 year old man presents to the Emergency Department complaining of a central band-like chest pain. He is obese with a history of type 2 diabetes. His 12 lead ECG is shown. What is the next management step in the Emergency Department?
A 47 year old man presents to the Emergency Department complaining of a central band-like chest pain. He is obese with a history of type 2 diabetes. His 12 lead ECG is shown. What is the next management step in the Emergency Department?
Answer:
There is horizontal ST depression in V1-3, with upright T waves. This could represent a posterior STEMI and needs to be confirmed with the posterior ECG leads V7-9. If posterior STEMI is confirmed the patient may be a candidate for pPCI and therefore confirming posterior STEMI takes priority.Acute Coronary Syndrome
Cardiology
Last Updated: 12th September 2022
Classification
Acute coronary syndrome (ACS) describes a group of clinical conditions, all of which usually present with chest pain or discomfort resulting from myocardial ischaemia:
- ST-segment-elevation myocardial infarction (STEMI)
- ST-segment elevation or new left bundle branch block (LBBB) present on ECG
- Non ST-segment-elevation acute coronary syndromes
- Non-ST-segment-elevation myocardial infarction (NSTEMI)
- Other ECG changes (e.g. ST-segment depression, T-wave inversion) or normal ECG with troponin release present
- Unstable angina (UA)
- Other ECG changes or normal ECG with troponin consistently negative
- Non-ST-segment-elevation myocardial infarction (NSTEMI)
Pathophysiology
In most cases this results from coronary artery disease and is initiated by the rupture or erosion of an atherosclerotic plaque within a coronary artery causing:
- acute thrombosis within the vessel lumen, often with haemorrhagic extension in the atherosclerotic plaque
- contraction of smooth muscle cells within the artery wall resulting in vasoconstriction that reduces the lumen of the artery
- associated partial or complete obstruction of the lumen, often with embolism of thrombus into the distal part of the vessel
This process results in a sudden and critical reduction in blood flow to the myocardium.
Risk Factors
- Family history of atherosclerosis
- Older age
- Male gender
- Smoking
- Diabetes mellitus
- Hypertension
- Hyperlipidaemia
- Sedentary lifestyle
- Obesity
Clinical Features
Determine whether chest pain is likely to be cardiac in origin by considering:
- the history of the chest pain
- the presence of cardiovascular factors
- any history of ischaemic heart disease and any previous treatment
- any previous investigations for chest pain
Initially assess people for any of the following symptoms, which may indicate an acute coronary syndrome:
- Pain in the chest or other areas (for example the arms, back, or jaw) lasting longer than 15 minutes
- Chest pain associated with nausea and vomiting, marked sweating, breathlessness, or a combination of these
- Chest pain associated with haemodynamic instability
- New onset chest pain or abrupt deterioration in previously stable angina; with recurrent chest pain occurring frequently and with little or no exertion, and with episodes often lasting longer than 15 minutes
- Do not use people's response to GTN to make a diagnosis
N.B. Some patient groups (e.g. elderly people, people with diabetes, females, people with renal disease and people during a perioperative period) are more likely to develop ACS with little or no chest discomfort; in such people, the dominant symptom may be breathlessness
| History | Likelihood Ratio |
|---|---|
| Increased likelihood | |
| Radiation to right arm/shoulder | 4.7 |
| Radiation to both arm/shoulder | 4.1 |
| Associated with exertion | 2.4 |
| Radiation to left arm | 2.3 |
| Associated with diaphoresis | 2 |
| Associated with nausea/vomiting | 1.9 |
| Worse than previous angina | 1.8 |
| Described as pressure | 1.3 |
| Decreased likelihood | |
| Described as pleuritic | 0.2 |
| Described as positional | 0.3 |
| Described as sharp | 0.3 |
| Reproducible with palpation | 0.3 |
| Inframammary location | 0.8 |
| Not associated with exertion | 0.8 |
Investigations
- 12-lead ECG
- Do not exclude an acute coronary syndrome when people have a normal resting 12-lead ECG
- Ischaemic ECG findings:
- Regional ST-segment elevation (2 mm ST-elevation in two contiguous chest leads or 1 mm ST-elevation in two contiguous limb leads)
- New left bundle branch block (LBBB)
- Regional ST-segment depression (> 0.5 mm) or deep T wave inversion (> 2 mm deep)
- Pathological Q waves
- Serum troponin (I or T)
- Use a validated tool to risk stratify patients at initial assessment for likelihood of acute myocardial infarction (AMI)
- For people at high or moderate risk of AMI:
- Perform high-sensitivity troponin tests as recommended
-
When interpreting high-sensitivity troponin measurements, take into account:
- the clinical presentation
- the time from onset of symptoms
- the resting 12-lead ECG findings
- the pre-test probability of NSTEMI
- the length of time since the suspected acute coronary syndrome
- the probability of chronically elevated troponin levels in some people
- that 99th percentile thresholds for troponin I and T may differ between sexes
- For people at low risk of AMI:
- Perform a second high-sensitivity troponin test as recommended if the first troponin test at presentation is positive
- Consider performing a single high-sensitivity troponin test only at presentation to rule out NSTEMI if the first troponin test is below the lower limit of detection (negative)
- N.B. Older standard troponin assays were taken at initial assessment and 10 - 12 hours after onset of symptoms
- Chest radiograph
- May diagnose complications of myocardial infarction such as pulmonary oedema, or exclude alternative diagnoses such as pneumothorax or pneumonia
- Echocardiography
- Left ventricular (LV) systolic function is directly related to prognosis and, in a person with acute chest pain, regional wall abnormalities increase the likelihood of ACS
- May allow prompt diagnosis of other conditions e.g. cardiomyopathies, valve disease, pericardial disease, aortic dissection and pulmonary embolism
- Can confirm or exclude right ventricular (RV) dilatation and impairment when extensive RV infarction is suspected
- Can be used to diagnose complications of AMI such as a ventricular septal defect and severe mitral regurgitation which may require urgent surgical correction
Diagnosis
A diagnosis of acute myocardial infarction is defined as the detection of the rise and/or fall of cardiac biomarkers (preferably troponin) with at least 1 value above the 99th percentile of the upper reference limit, together with evidence of myocardial ischaemia with at least one of the following:
- Symptoms of ischaemia
- ECG changes indicative of ischaemia (new ST-segment or T-wave changes or new LBBB)
- Development of pathological Q waves in the ECG
- Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality
- Identification of an intracoronary thrombus by angiography
When a raised troponin level is detected in people with a suspected acute coronary syndrome, reassess to exclude other causes for raised troponin (for example, myocarditis, aortic dissection or pulmonary embolism) before confirming the diagnosis of acute coronary syndrome.
Localisation of Lesion in STEMI
The ECG provides some information about the site and extent of myocardial damage in acute myocardial infarction, particularly in STEMI. The ECG changes that may occur in NSTEMI are less-clearly related to the site of myocardial damage than the changes in STEMI.
- A septal infarct shows changes in the V1 - V2 leads, and typically involves the left anterior descending artery.
- An anterior infarct shows changes in the V3 - V4 leads, and typically involves the left anterior descending artery.
- A lateral infarct shows changes in leads V5 - V6, I, aVL, and typically involves the left circumflex artery or diagonal branch of the left anterior descending artery.
- An anteroseptal infarct shows changes in the V1 - V4 leads and typically involves the left anterior descending artery.
- An anterolateral infarct shows changes in leads I, aVL, V3 - V6 (and reciprocal changes in leads II, III, aVF) and typically involves the left anterior descending or the left circumflex artery.
- An inferior infarct shows changes in leads II, III, aVF (and reciprocal changes in leads I, aVL) and typically involves the right coronary artery.
- A posterior infarct shows reciprocal changes in leads V1 - V3 and requires placement of posterior leads (V7 - V9) to identify ST-elevation - it typically involves the right coronary artery or the left circumflex artery.
| Affected myocardial area | Leads with ST-segment elevation | Occluded coronary artery |
|---|---|---|
| Septal | V1 - V2 | Proximal LAD |
| Anterior | V3 - V4 | LAD |
| Lateral | V5 - V6, I, aVL | LCX |
| Anteroseptal | V1 - V4 | LAD |
| Anterolateral | V3 - V6, I, aVL (R: II, III, aVF) | LAD or LCX |
| Inferior | II, III, aVF (R: I, aVL) | RCA |
| Posterior/Posterolateral | R: V1 - V3 (P: V7 - V9) | RCA or LCX |
*RCA = right coronary artery, LAD = left anterior descending coronary artery, LCX = left circumflex coronary artery, R = reciprocal ST-depression, P = posterior leads
Immediate Management of ACS
Immediate treatment for ACS comprises:
- Aspirin 300 mg orally, crushed or chewed (unless there is clear evidence of allergy)
- Sublingual glyceryl trinitrate, spray or tablet (unless the patient is hypotensive)
- Oxygen if the patient is hypoxic (sats < 94% on air), aim for sats of 94 - 98% (unless COPD)
- Analgesia with IV opioid, titrated to control symptoms whilst avoiding sedation or respiratory depression, and given with an antiemetic
Management of STEMI
- Coronary reperfusion therapy
- Immediately assess eligibility (irrespective of age, ethnicity or sex) for coronary reperfusion therapy and if eligible, deliver coronary reperfusion therapy as quickly as possible
- Presentation within 12 hours:
- Offer coronary angiography, with follow-on primary percutaneous coronary intervention (PCI) if indicated, as the preferred coronary reperfusion strategy for people with acute STEMI if presentation is within 12 hours of onset of symptoms AND primary PCI can be delivered within 120 minutes of the time when fibrinolysis could have been given
- Offer fibrinolysis to people with acute STEMI presenting within 12 hours of onset of symptoms if primary PCI cannot be delivered within 120 minutes of the time when fibrinolysis could have been given
- Presentation beyond 12 hours:
- Consider coronary angiography, with follow-on primary PCI if indicated, for people with acute STEMI presenting more than 12 hours after the onset of symptoms if there is evidence of continuing myocardial ischaemia or of cardiogenic shock
Primary percutaneous coronary intervention
- In addition to aspirin, all patients should be given one of the platelet ADP receptor blockers prior to PCI using a loading dose (clopidogrel, prasugrel, ticagrelor)
- Anticoagulation with unfractionated or low molecular weight heparin is given in the catheter laboratory and in high-risk cases a glycoprotein IIb/IIIa inhibitor may also be given. Bivalirudin, a direct thrombin inhibitor may be chosen as an alternative to heparin.
Fibrinolytic therapy
- Additional antithrombin therapy must be given to minimise the risk of further thrombotic occlusion. In addition to aspirin, all patient should be given a loading dose of clopidogrel and antithrombin therapy using unfractionated or low molecular weight heparin.
- An ECG should be recorded 60–90 minutes after administration of fibrinolysis. For those who have residual ST-segment elevation suggesting failed coronary reperfusion offer immediate coronary angiography, with follow-on PCI if indicated and do not repeat fibrinolytic therapy.
- If a person has recurrent myocardial ischaemia after fibrinolysis, seek immediate specialist cardiological advice and, if appropriate, offer coronary angiography, with follow-on PCI if indicated.
- Consider coronary angiography during the same hospital admission for people who are clinically stable after successful fibrinolysis.
Management of NSTEMI/UA
- Initial drug treatment
- Aspirin
- Offer aspirin as soon as possible to all patients (initial loading dose 300 mg) and continue indefinitely (75 mg daily) unless contraindicated by bleeding risk or aspirin hypersensitivity.
- Antithrombin therapy
- Offer fondaparinux to patients who do not have a high bleeding risk, unless coronary angiography is planned within 24 hours of admission.
- Offer unfractionated heparin as an alternative to fondaparinux to patients who are likely to undergo coronary angiography within 24 hours of admission or in renal impairment.
- Aspirin
- Further drug treatment
- As soon as the diagnosis of unstable angina or NSTEMI is made, and aspirin and antithrombin therapy have been offered, formally assess individual risk of future adverse cardiovascular events using an established risk scoring system that predicts 6-month mortality (for example, GRACE).
- Clopidogrel
- Offer a loading dose of 300 mg clopidogrel in addition to aspirin to patients with a predicted 6-month mortality of more than 1.5% and no contraindications (for example, an excessive bleeding risk).
- Offer a 300-mg loading dose of clopidogrel to all patients with no contraindications who may undergo PCI within 24 hours of admission to hospital.
- Offer clopidogrel as a treatment option for up to 12 months to people who have had an NSTEMI, regardless of treatment.
- ADP receptor blocker alternatives to clopidogrel include prasugrel or ticagrelor
- Glycoprotein inhibitors
- Consider intravenous eptifibatide or tirofiban as part of the early management for patients who have an intermediate or higher risk of adverse cardiovascular events (predicted 6-month mortality above 3.0%), and who are scheduled to undergo angiography within 96 hours of hospital admission.
- Coronary angiography
- Offer conservative management without early coronary angiography to patients with a low risk of adverse cardiovascular events (predicted 6-month mortality 3.0% or less).
- Offer coronary angiography (with follow-on PCI if indicated) to patients initially assessed to be at low risk of adverse cardiovascular events (predicted 6-month mortality 3.0% or less) if ischaemia is subsequently experienced or is demonstrated by ischaemia testing.
- Offer coronary angiography (with follow-on PCI if indicated) within 96 hours of first admission to hospital to patients who have an intermediate or higher risk of adverse cardiovascular events (predicted 6-month mortality above 3.0%) if they have no contraindications to angiography (such as active bleeding or comorbidity). Perform angiography as soon as possible for patients who are clinically unstable or at high ischaemic risk.
Secondary Prevention
- Antithrombotic therapy
- Low-dose (75 mg) aspirin daily for life
- Clopidogrel 75 mg daily/prasugrel 10 mg daily/ticagrelor 90 mg twice daily for 1 year for patients with high risk ACS and all those undergoing PCI
- Preservation of left ventricular function
- Treatment after AMI with an ACE inhibitor can reduce the remodelling that contributes to left ventricular dilatation and impairment; the use of ACEI therapy in adequate dose can reduce the risk and severity of subsequent heart failure and the risk of future MI
- Beta-adrenoceptor blockade
- Treatment with a beta-blocker, started early after AMI and continued, has been shown to reduce mortality
- Reduction of cholesterol
- Statins reduce future coronary events by at least 30%; a low-fat, high-fibre diet and regular exercise will complement cholesterol suppression by drugs
- Antihypertensive therapy
- Effective control of raised blood pressure reduces the risk of stroke, heart failure and future coronary events
- Smoking cessation
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |