

Cardiology
This was previously featured in an exam
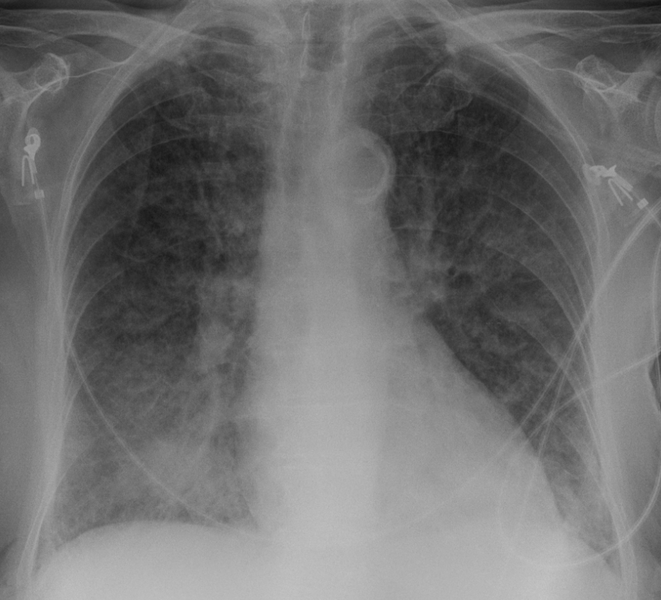
A 65 year old man, with a history of diabetes mellitus, presents to ED with complaints of a worsening cough and shortness of breath over the past 4 weeks. His observations are: BP 135/90, HR 110, RR 24, SpO2 92% OA. His COVID-19 PCR is negative. His chest x-ray is shown. What is the most appropriate management in this patient?
Answer:
The x-ray shows pulmonary oedema. The priority in the treatment of acute pulmonary oedema is intravenous furosemide.Cardiac Failure
Cardiology
Last Updated: 28th February 2022
Heart failure is defined clinically as a syndrome in which patients have symptoms and signs resulting from an abnormality of cardiac structure and/or function. Acute heart failure refers to rapid onset or worsening of symptoms and/or signs of heart failure, requiring urgent evaluation and treatment.
Causes of heart failure
Many different conditions can lead to heart failure with possible overlap between categories. Causes include:
- Myocardial disease
- Coronary artery disease (most common)
- Hypertension
- Cardiomyopathies e.g. familial, infective, immune-mediated, toxins (for example alcohol or cocaine), pregnancy, infiltrative (for example sarcoidosis, amyloidosis, haemochromatosis, connective tissue disease)
- Valvular heart disease (for example aortic stenosis)
- Pericardial disease
- Constrictive pericarditis
- Pericardial effusion
- Congenital heart disease
- Arrhythmias (for example atrial fibrillation and other tachyarrhythmias)
- High output states:
- Anaemia
- Thyrotoxicosis
- Phaeochromocytoma
- Septicaemia
- Liver failure
- Arteriovenous shunts
- Paget's disease
- Thiamine (vitamin B1) deficiency
- Volume overload
- End-stage chronic kidney disease
- Nephrotic syndrome
- Obesity
- Drugs including:
- Alcohol
- Cocaine
- Nonsteroidal anti-inflammatory drugs, beta-blockers, and calcium-channel blockers (may worsen pre-existing heart failure)
Clinical features of heart failure
Take a careful and detailed history, and perform a clinical examination and tests to confirm the presence of heart failure.
- Symptoms
- Breathlessness — on exertion, at rest, on lying flat (orthopnoea), nocturnal cough, or waking from sleep (paroxysmal nocturnal dyspnoea)
- Coughing (rarely with frothy blood-stained sputum)
- Fluid retention (ankle swelling, bloated feeling, abdominal swelling, or weight gain)
- Fatigue, decreased exercise tolerance, or increased recovery time after exercise
- Lightheadedness or history of syncope
- Signs
- Tachycardia (heart rate over 100 beats per minute) and pulse rhythm
- A laterally displaced apex beat, heart murmurs, and third or fourth heart sounds (gallop rhythm)
- Hypertension
- Raised jugular venous pressure
- Enlarged liver (due to engorgement)
- Respiratory signs such as tachypnoea, basal crepitations, wheeze and pleural effusions
- Dependent oedema (legs, sacrum), ascites
- Poor peripheral circulation
Differential diagnosis
A number of conditions can present with symptoms and signs similar to heart failure including:
- Conditions causing breathlessness such as:
- Chronic obstructive pulmonary disease
- Asthma
- Pulmonary embolism
- Lung cancer
- Anxiety
- Conditions causing peripheral oedema such as:
- Prolonged inactivity or venous insufficiency causing dependent oedema
- Nephrotic syndrome
- Drugs (for example dihydropyridine calcium-channel blockers, nonsteroidal anti-inflammatory drugs)
- Hypoalbuminaemia (from renal or hepatic disease)
- Pelvic tumour
- Other conditions such as:
- Obesity
- Severe anaemia or thyroid disease
- Bilateral renal artery stenosis
Investigations in acute heart failure
- Natriuretic peptide testing
- In people presenting with new suspected acute heart failure, use a single measurement of serum natriuretic peptides (B‑type natriuretic peptide [BNP] or N‑terminal pro‑B‑type natriuretic peptide [NT‑proBNP]) and the following thresholds to rule out the diagnosis of heart failure
- BNP less than 100 ng/litre
- NT‑proBNP less than 300 ng/litre.
- In people presenting with new suspected acute heart failure, use a single measurement of serum natriuretic peptides (B‑type natriuretic peptide [BNP] or N‑terminal pro‑B‑type natriuretic peptide [NT‑proBNP]) and the following thresholds to rule out the diagnosis of heart failure
- Echo
- In people presenting with new suspected acute heart failure with raised natriuretic peptide levels, perform transthoracic Doppler 2D echocardiography to establish the presence or absence of cardiac abnormalities.
- In people presenting with new suspected acute heart failure, consider performing transthoracic Doppler 2D echocardiography within 48 hours of admission to guide early specialist management.
- ECG:
- To look for e.g.
- Signs of heart failure e.g. ventricular strain pattern
- Ischaemia
- Arrhythmia
- To look for e.g.
- Chest x-ray
- To look for signs of heart failure
- Upper lobe diversion (distension of upper pulmonary veins)
- Kerley B septal lines (fluid in the interstitium)
- Bat’s wing hilar shadowing (blurred margins of the hilar vessels)
- Fluid in interlobar fissures
- Peribronchial/perivascular cuffing and nodules
- Pleural effusions
- Cardiomegaly
- To look for signs of heart failure
- Blood tests
- renal function profile
- thyroid function profile
- liver function profile
- lipid profile
- glycosylated haemoglobin (HbA1c)
- full blood count
- troponin
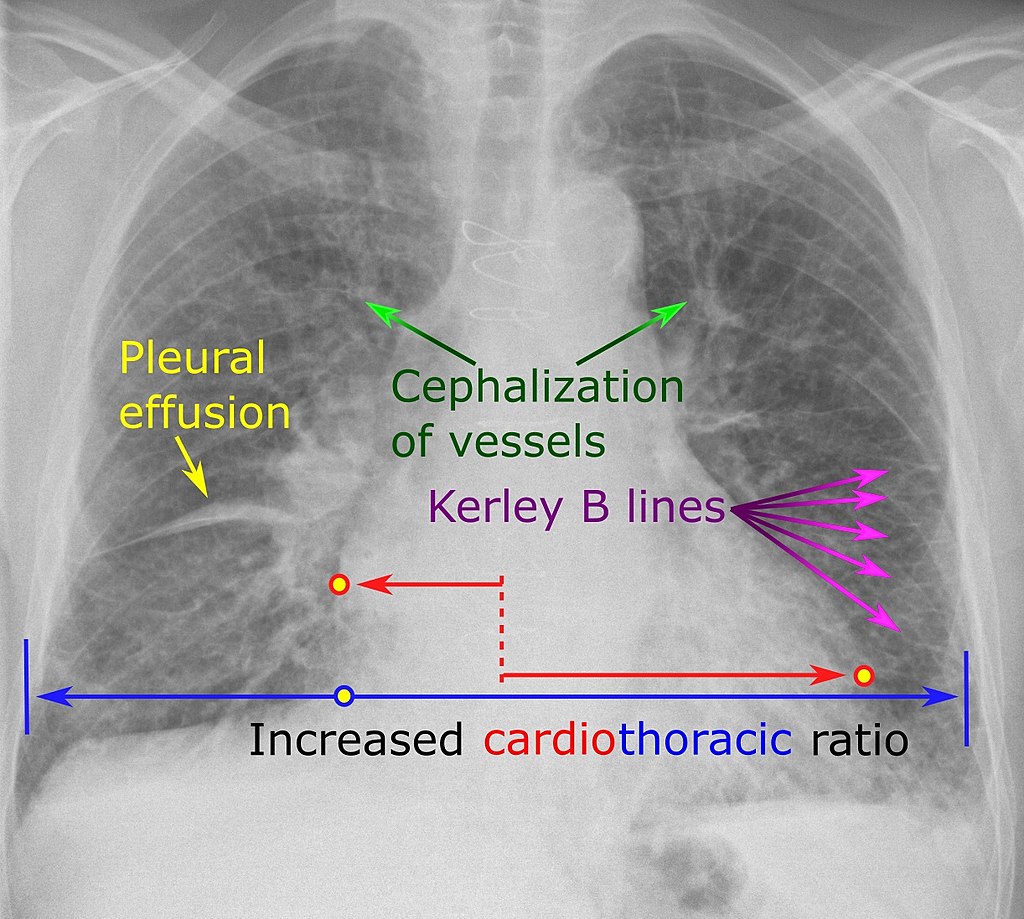
Signs of congestive heart failure. (Image by Mikael Häggström, CC0, via Wikimedia Commons)
Management of acute heart failure
Acute heart failure can present as new‑onset heart failure in people without known cardiac dysfunction, or as acute decompensation of chronic heart failure.
- Initial pharmacological treatment:
- Opiates
- Do not routinely offer opiates to people with acute heart failure.
- Diuretics
- Offer intravenous diuretic therapy to people with acute heart failure. Start treatment using either a bolus or infusion strategy.
- For people already taking a diuretic, consider a higher dose of diuretic than that on which the person was admitted unless there are serious concerns with patient adherence to diuretic therapy before admission.
- Closely monitor the person's renal function, weight and urine output during diuretic therapy.
- Nitrates
- Do not routinely offer nitrates to people with acute heart failure.
- If intravenous nitrates are used in specific circumstances, such as for people with concomitant myocardial ischaemia, severe hypertension or regurgitant aortic or mitral valve disease, monitor blood pressure closely in a setting where at least level 2 care can be provided.
- Do not offer sodium nitroprusside to people with acute heart failure.
- Inotropes/vasopressors
- Do not routinely offer inotropes or vasopressors to people with acute heart failure.
- Consider inotropes or vasopressors in people with acute heart failure with potentially reversible cardiogenic shock. Patients with a systolic BP below 90 mmHg or a drop of mean arterial pressure of more than 30 mmHg with a pulse rate above 60 bpm and/or low urine output (<0.5 mL/kg/hour) are defined as being in cardiogenic shock. Administer these treatments in a cardiac care unit or high dependency unit or an alternative setting where at least level 2 care can be provided.
- Opiates
- Initial non-pharmacological treatment:
- Oxygen
- High flow oxygen is recommended in patients with a capillary oxygen saturation <90% or PaO₂ <60 mmHg (8.0 kPa) to correct hypoxaemia.
- Non-invasive ventilation
- If a person has cardiogenic pulmonary oedema with severe dyspnoea and acidaemia consider starting non‑invasive ventilation without delay:
- at acute presentation or
- as an adjunct to medical therapy if the person's condition has failed to respond.
- If a person has cardiogenic pulmonary oedema with severe dyspnoea and acidaemia consider starting non‑invasive ventilation without delay:
- Invasive ventilation
- Consider invasive ventilation in people with acute heart failure that, despite treatment, is leading to or is complicated by:
- respiratory failure or
- reduced consciousness or physical exhaustion.
- Consider invasive ventilation in people with acute heart failure that, despite treatment, is leading to or is complicated by:
- Ultrafiltration
- Do not routinely offer ultrafiltration to people with acute heart failure.
- Consider ultrafiltration for people with confirmed diuretic resistance.
- Oxygen
- Treatment after stabilisation:
- Beta-blocker
- In a person presenting with acute heart failure who is already taking beta‑blockers, continue the beta‑blocker treatment unless they have a heart rate less than 50 beats per minute, second or third degree atrioventricular block, or shock.
- Start or restart beta‑blocker treatment during hospital admission in people with acute heart failure due to left ventricular systolic dysfunction, once their condition has been stabilised – for example, when intravenous diuretics are no longer needed.
- Ensure that the person's condition is stable for typically 48 hours after starting or restarting beta‑blockers and before discharging from hospital.
- ACE inhibitor
- Offer an angiotensin‑converting enzyme inhibitor (or angiotensin receptor blocker if there are intolerable side effects) and an aldosterone antagonist during hospital admission to people with acute heart failure and reduced left ventricular ejection fraction. If the angiotensin‑converting enzyme inhibitor (or angiotensin receptor blocker) is not tolerated an aldosterone antagonist should still be offered.
- Beta-blocker
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |