

Cardiology
This was previously featured in an exam
This was previously featured in an exam
Question 29 of 148
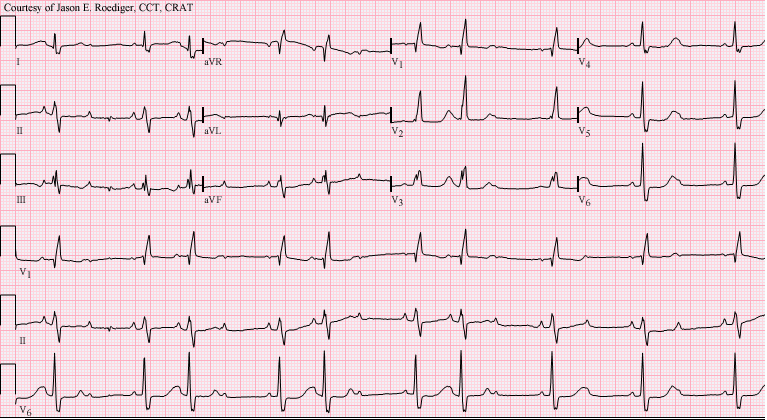
A 76 year old woman is brought to the Emergency Department after having a syncopal episode at home. She describes multiple similar episodes in the previous week. Her observations at triage are recorded as:
- Heart rate: 50 beats/minute
- Blood pressure: 135/67 mmHg
- Respiratory rate: 16 breaths/minute
An ECG is performed. What is the diagnosis?
Answer:
This is second degree (Mobitz Type II) heart block where there is intermittent dropping of ventricular conduction. Identification of a Mobitz type II AV block, with symptoms, is an indication for insertion of a permanent pacemaker.Heart Block and Conduction Abnormalities
Cardiology
Last Updated: 16th May 2023
Atrioventricular (AV) heart block
- First degree AV block
- Prolongation of PR interval (>0.2s)
- Second degree AV block Mobitz type I
- Progressive prolongation of PR interval after each successive P wave with eventual dropped ventricular conduction
- Second degree AV block Mobitz type II
- Constant (often prolonged) PR interval with random intermittent dropping of ventricular conduction
- Second degree AV block (2:1 type) block
- Alternate P waves not conducted to ventricles; alternate P waves not followed by QRS complex
- Third degree (complete) AV block
- Complete dissociation between atria and ventricles; no relationship between P waves and QRS complex
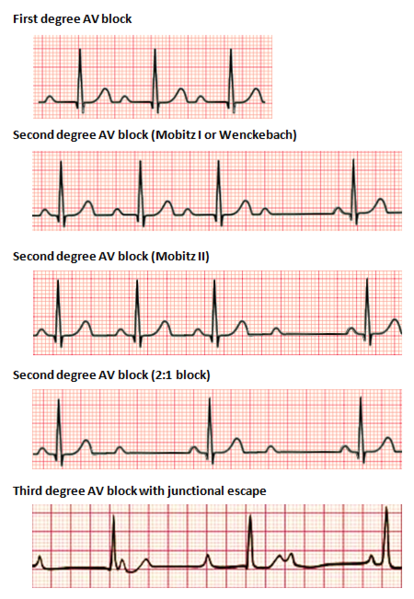
Types of Heart Block. (Image by Npatchett, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons)
Bundle Block
- Left anterior fascicular block (LAFB)
- Left axis deviation (leads I/avL are positive, leads II/III/avF are negative)
- qR complexes in I, aVL (small Q waves and tall R waves)
- rS complexes in II, III, aVF (small R waves and deep S waves)
- No evidence of LVH
- Left posterior fascicular block (LPFB)
- Right axis deviation (leads I/avL are negative, leads II/III/avF are positive)
- rS complexes in I, aVL (small R waves and deep S waves)
- qR complexes in II, III, aVF (small Q waves and tall R waves)
- No evidence of RVH
- Left bundle branch block (LBBB)
- QRS duration > 120 ms
- Dominant S wave in V1
- Broad monophasic R wave in lateral leads (I, aVL, V5-6)
- Absence of Q waves in lateral leads
- Prolonged R wave peak time > 60ms in leads V5-6
- Right bundle branch block (RBBB)
- QRS duration > 120 ms
- RSR pattern in in V1-V3 (M-shaped QR complex)
- Wide, slurred S wave in lateral leads (I, aVL, V5-6)
- Bifascicular block presents with one of two ECG patterns:
- RBBB + LAFB manifests as left axis deviation
- RBBB + LPFB manifests as right axis deviation
- Trifascicular block
- True trifascicular block presents with one of two ECG patterns:
- 3rd degree AV block + RBBB + LAFB
- 3rd degree AV block + RBBB + LPFB
- Clinically, trifascicular block is most commonly used to describe:
- bifascicular block + 1st degree AV block or 2nd degree AV block
- True trifascicular block presents with one of two ECG patterns:
*LAD = left axis deviation, RAD = right axis deviation
VT vs SVT with aberrancy
Differentiating between SVT with aberrancy versus VT can be very difficult.
Clinical factors associated with VT or SVT:
- The likelihood of VT is increased with:
- Age > 35 (positive predictive value of 85%)
- Structural heart disease
- Ischaemic heart disease
- Previous MI
- Family history of sudden cardiac death (suggesting conditions such as HOCM, congenital long QT syndrome, Brugada syndrome or arrhythmogenic right ventricular dysplasia that are associated with episodes of VT)
- The likelihood of SVT with aberrancy is increased if:
- Previous ECGs show a bundle branch block pattern with identical morphology to the broad complex tachycardia
- Previous ECGs show evidence of WPW (short PR < 120ms, broad QRS, delta wave)
- The patient has a history of paroxysmal tachycardias that have been successfully terminated with adenosine or vagal manoeuvres
ECG features associated with VT or SVT:
- Electrocardiographic features that increase the likelihood of VT include:
- Absence of typical RBBB or LBBB morphology
- Extreme axis deviation (“northwest axis”): QRS positive in aVR and negative in I and aVF
- Very broad complexes > 160ms
- AV dissociation: P and QRS complexes at different rates (P waves are often superimposed on QRS complexes and may be difficult to discern)
- Capture beats: Occur when the sinoatrial node transiently “captures” the ventricles in the midst of AV dissociation, producing a QRS complex of normal duration
- Fusion beats: Occur when a sinus and ventricular beat coincide to produce a hybrid complex
- Positive or negative concordance throughout the precordial leads (no rS complexes seen)
- RSR’ complexes with a taller left rabbit ear (in contrast to RBBB, where the right rabbit ear is taller)
- Brugada sign: Distance from onset of R wave to nadir of S wave is > 100ms in leads V1-6
- Josephson sign: Notching/slurring near the nadir of the S wave
Brugada criteria for ventricular tachycardia:
- Is there an absence of an RS complex in all precordial leads?
- If yes = VT
- If no = next question
- Is the R to S interval >100 msec (2.5 small boxes) in one precordial lead?
- If yes = VT
- If no = next question
- Is there atrioventricular (AV) dissociation?
- If yes = VT
- If no = next question
- Is there morphology criteria for VT present in precordial leads V1/V2 and V6?
- If yes = VT
- If no = SVT with aberrancy
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |