

Cardiology
This was previously featured in an exam
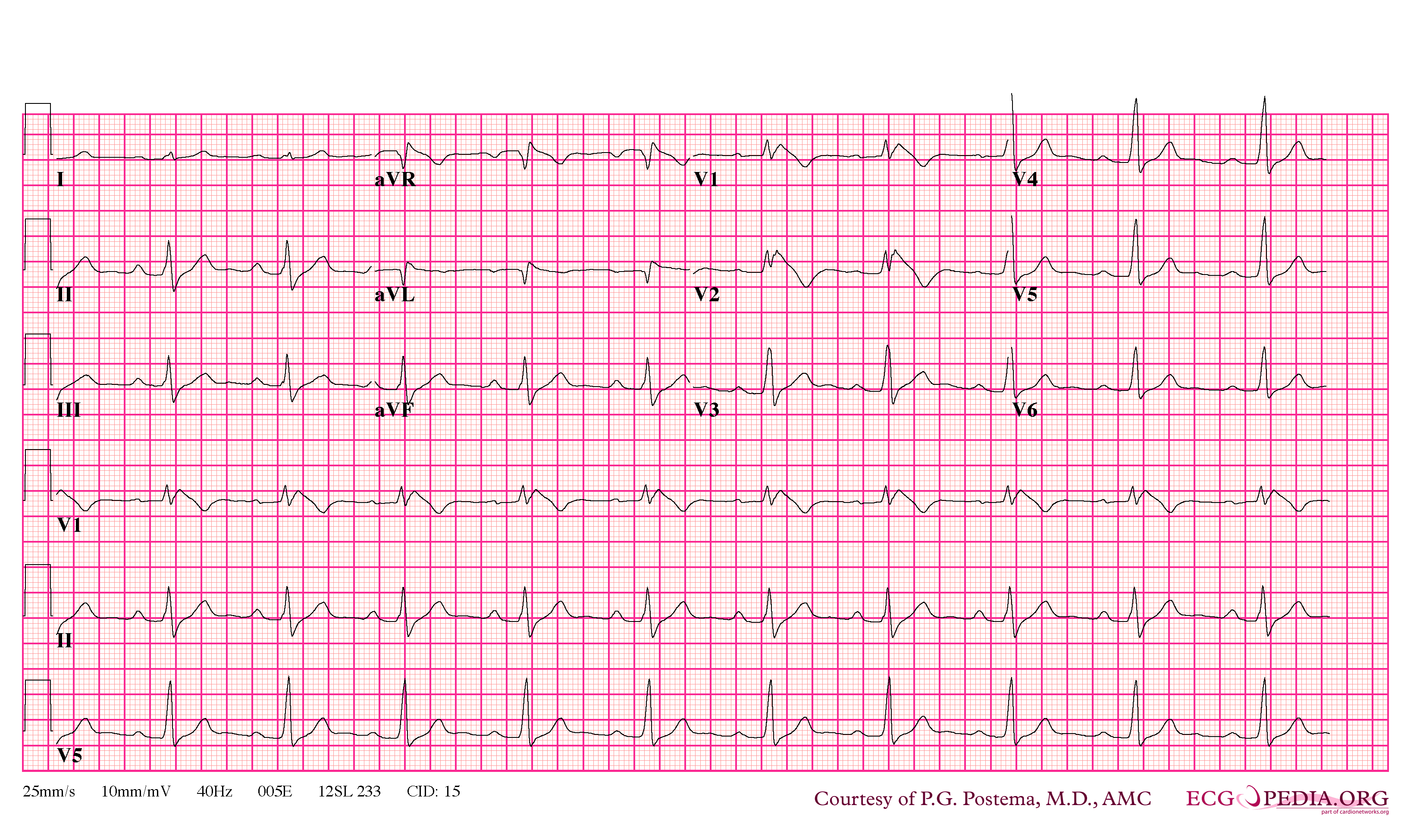
A 39 year old man presents to ED complaining of syncopal episodes. He is concerned as his father died suddenly and unexpectedly when he was 42. What is the most likely diagnosis?
Answer:
The ECG shows the Brugada Type 1 pattern in leads V1 and V2 with prominent coved ST-segment elevation displaying J-point amplitude, followed by a negative T wave. Together with the clinical history of sudden cardiac death in a family member younger than 45 years old, and a personal history of syncope, the diagnosis is likely Brugada syndrome.Brugada Syndrome
Cardiology
Last Updated: 17th November 2022
Brugada syndrome (BS), first described in 1992, is an inherited arrhythmogenic disease characterised by coved-type ST-segment elevation in right precordial leads and an increased risk of sudden cardiac death (SCD) due to ventricular fibrillation (VF). Approximately 80% of the affected individuals are men and the onset of symptoms typically occurs at a mean age of 40.
ECG pattern
Three repolarisation patterns are associated with BS when found in more than one right precordial leads (V1 to V3). Type 1 is the only ECG diagnostic pattern of BS, while types 2 and 3 should only be considered suggestive of the disease.
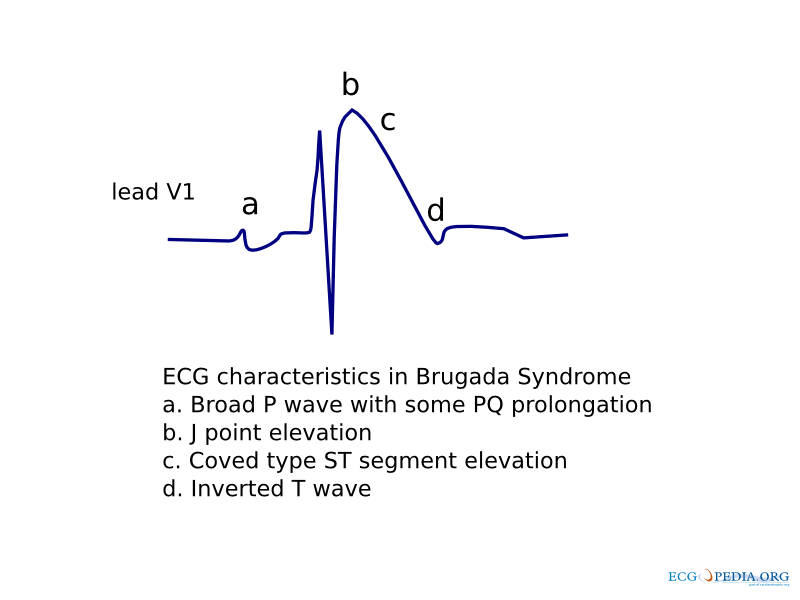
- Type 1
- It is characterised by a prominent coved ST-segment elevation displaying J-point amplitude or ST-segment elevation ≥2 mm, followed by a negative T wave.
- Type 2
- It has ≥2 mm J-point elevation, ≥1 mm ST-segment elevation and a saddleback appearance, followed by a positive or biphasic T-wave.
- Type 3
- It has either a saddleback or coved appearance, but with an ST-segment elevation <1 mm.
A drug challenge with class I antiarrhythmic drugs (AAD) for the diagnosis of BS is indicated in cases in which the disease is suspected, but in which the basal ECG is normal (e.g. familial screening) or suspicious, but not diagnostic (types 2 or 3). Flecainide, ajmaline, procainamide, dispyramide, propafenone and pilsicainide have been used to unmask BS. A drug challenge is only considered positive when a conversion to the diagnostic type 1 occurs.
It is recommended to place the right precordial leads up to the second intercostals space because it may increase the sensitivity of the ECG (basal and during drug challenge with Class I AAD) for detecting the diagnostic BS pattern.
Diagnosis
Many conditions may develop ST-segment elevation, mimicking the BS ECG pattern. In order to attain the diagnosis of BS, they should be carefully excluded. It is also important to be aware that some drugs may also produce a Brugada-like ST-segment elevation.
Once a type 1 ECG has been observed in more than one precordial lead and other conditions have been excluded that may account for it, clinical data should be sought that supports the diagnosis of BS. There are three kinds of clinical criteria for the disease:
- Data from the family history:
- SCD in a family member younger than 45.
- ECG type 1 in family members.
- Arrhythmia-related symptoms:
- Syncope.
- Seizures.
- Nocturnal agonal respiration.
- Documented ventricular arrhythmias:
- Polymorphic ventricular tachycardia (PVT).
- Ventricular fibrillation (VF).
BS is definitely diagnosed when the patient presents: 1) a type 1 ECG (either spontaneously or elicited by a drug challenge) and 2) at least one of the above-mentioned clinical criteria. If a type 1 ECG is observed in the absence of any clinical criteria, this should be referred to as 'idiopathic Brugada ECG pattern' and not as BS.
Risk stratification
Once the diagnosis of BS is made, the next step is risk stratification for which the main objective is the accurate identification and treatment of individuals at high risk of SCD (25% of the total population with BS will experience SCD or VF during their lifetimes. To date, some markers of high risk in BS patients have been clearly identified, but other issues still remain controversial.
- Survivors of SCD are at high risk of recurrence or life-threatening arrhythmias months follow-ups and should receive an ICD.
- Syncope is also a marker of high risk of presenting ventricular arrhythmias, and should receive an ICD, after non-cardiac causes of this symptom have been carefully ruled out.
- Spontaneous ECG type 1 is not an independent predictor of ventricular arrhythmias in multivariate analysis of the largest registries on the subject, but it still identified a subgroup of patients with a higher risk of future arrhythmic events when combined with a history of syncope and inducibility during electrophysiological (EP) study.
- Males show a tendency to develop more arrhythmic events than women and have a worse prognosis during follow-up.
Management
To date, the only proven effective therapeutic strategy for the prevention of SCD in BS patients is the implantable cardioverter-defibrillator (ICD). These patients present a considerably high rate of inappropriate shocks, mostly due to sinus tachycardia, supraventricular tachyarrhythmias and lead complications; emphasising the importance of a careful ICD programming.
Other recommendations:
- It is recommended that BS patients should avoid all drugs that may induce a type 1 class ECG.
- As fever may elicit the diagnostic ECG pattern and has also been recognised as a trigger of ventricular arrhythmias in BS, patients should be encouraged to treat it aggressively.
- Patients must contact their cardiologist immediately in case of presenting syncope, seizures or nocturnal agonal respiration.
- Family screening of BS is strongly recommended in first-degree relatives (BS is an inherited disease transmitted in an autosomal-dominant way).
- All patients must have regular follow-ups in order to identify the development of symptoms.
- Genetic testing, when available, is recommended to support clinical diagnosis, early detection of other affected family members and for research purposes. But diagnosis should not be based on it because it still has a low diagnostic yield.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |