

Maxillofacial & Dental
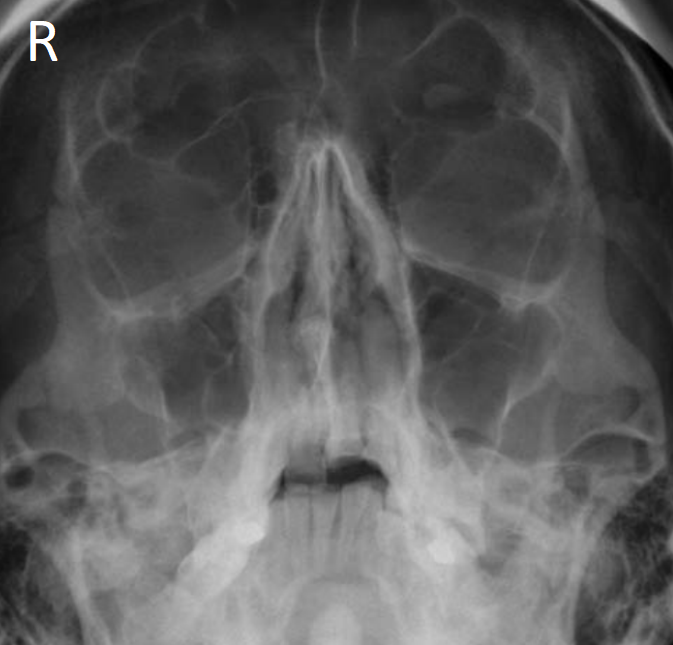
A 32 year old is brought to the Emergency Department after being found collapsed in the street. Enroute to the Emergency Department his GCS improves to 15 and he tells you he has been drinking heavily and thinks he fell. He has evidence of trauma to the face. Which of the following best describes the findings on this x-ray?
Answer:
In zygomaticomaxillary complex fractures, the following fracture components are usually identified:- Fracture of the zygomatic arch and/or diastasis of the zygomaticotemporal suture
- Fracture of the lateral orbital rim and/or diastasis of the frontozygomatic suture
- Fractures of the inferior orbital rim and maxillary sinus wall and/or diastasis of the zygomaticomaxillary suture
Zygomaticomaxillary Complex Injury
Maxillofacial & Dental
Last Updated: 21st March 2021
Clinical anatomy
The zygoma forms a large part of the anterolateral wall of the orbit, the lateral margin of the infraorbital rim and the anterior segment of the zygomatic arch. The zygoma has four bony attachments to the skull:
- A superior attachment to the frontal bone (frontozygomatic suture line)
- A medial attachment to the maxilla (zygomaticomaxillary suture line)
- A lateral attachment to the temporal bone (zygomaticotemporal suture line)
- A deep attachment to the greater wing of the sphenoid bone (zygomaticosphenoidal suture line)
This complex is referred to as the zygomaticomaxillary complex (ZMC). The malar eminence corresponds to the central portion of the zygomaticomaxillary complex.
In zygomaticomaxillary complex fractures, the following fracture components are usually identified:
- Fracture of the zygomatic arch and/or diastasis of the zygomaticotemporal suture
- Fracture of the lateral orbital rim and/or diastasis of the frontozygomatic suture
- Fractures of the inferior orbital rim and maxillary sinus wall and/or diastasis of the zygomaticomaxillary suture
Immediately below the infraorbital margin lies the infraorbital foramen, through which passes the infraorbital nerve (part of the maxillary division of the trigeminal nerve). The nerve’s location makes it very vulnerable to both direct injury, and involvement in ZMC fractures. Additionally, the fracture components may result in impingement of the temporalis muscle with trismus.
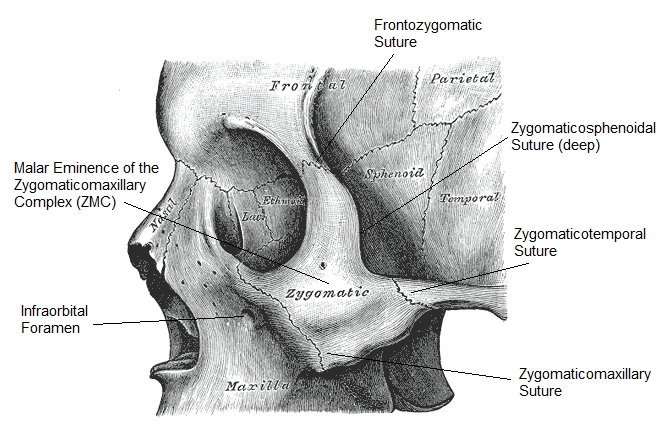
Zygomaticomaxillary complex (ZMC). (Image modified by FRCEM Success. Original by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
Management
The vast majority of ZMC fractures can be managed expectantly until local swelling subsides, and reviewed by a maxillofacial surgeon at a time guided by local policy.
Any indication of eye involvement (e.g. reduced visual acuity or diplopia) is an indication for urgent referral to a maxillofacial surgeon and/or an ophthalmologist. Suspected infraorbital nerve involvement is not an indication for urgent referral.
There is no good evidence that antibiotics should be routinely prescribed in ZMC fracture, although there is a well documented, but rare, risk of orbital cellulitis. Local policy should be followed.
Discharge advice
Patients should be given general advice regarding their injury including:
- Avoidance of nose blowing as this may produce surgical emphysema
- Not to occlude the nose when sneezing
- Application of ice packs to the area to reduce swelling
- Taking regular analgesia
- General head injury advice
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |