

Maxillofacial & Dental
This was previously featured in an exam
An 18 year old rugby player presents to the Emergency Department after getting punched during a game. He was not wearing any dental protection at the time and his central upper left incisor (UL1) is missing. His teammates found the missing tooth and have brought it to the Emergency Department in milk. Which of the following immediate management steps is correct?
Answer:
- The tooth should be held in a physiologically acceptable medium (saliva or milk) before re-implantation.
- It is important to hold the tooth at the crown only (the part that is normally visible in the mouth) and to avoid touching the root surface.
- Saline should be used to briefly clean debris from the root of the tooth and also to irrigate the socket to remove any blood clots that may be present here (allowing for revascularisation of the tooth).
- The tooth should be gently placed back into the socket, and splinting carried out, ensuring that the tooth is orientated correctly in the correct socket.
- Antibiotics should be given and a tetanus booster considered.
- Early and prompt referral to dental surgeon or maxillofacial surgeon is required.
- It is worth noting that teeth that are outside of the mouth for more than 60 minutes are more likely to fail and undergo root resorption (breakdown) or ankylosis (fusion of root to the bone) and ultimately fail.
Dental Trauma
Maxillofacial & Dental
Last Updated: 30th January 2024
Clinical anatomy
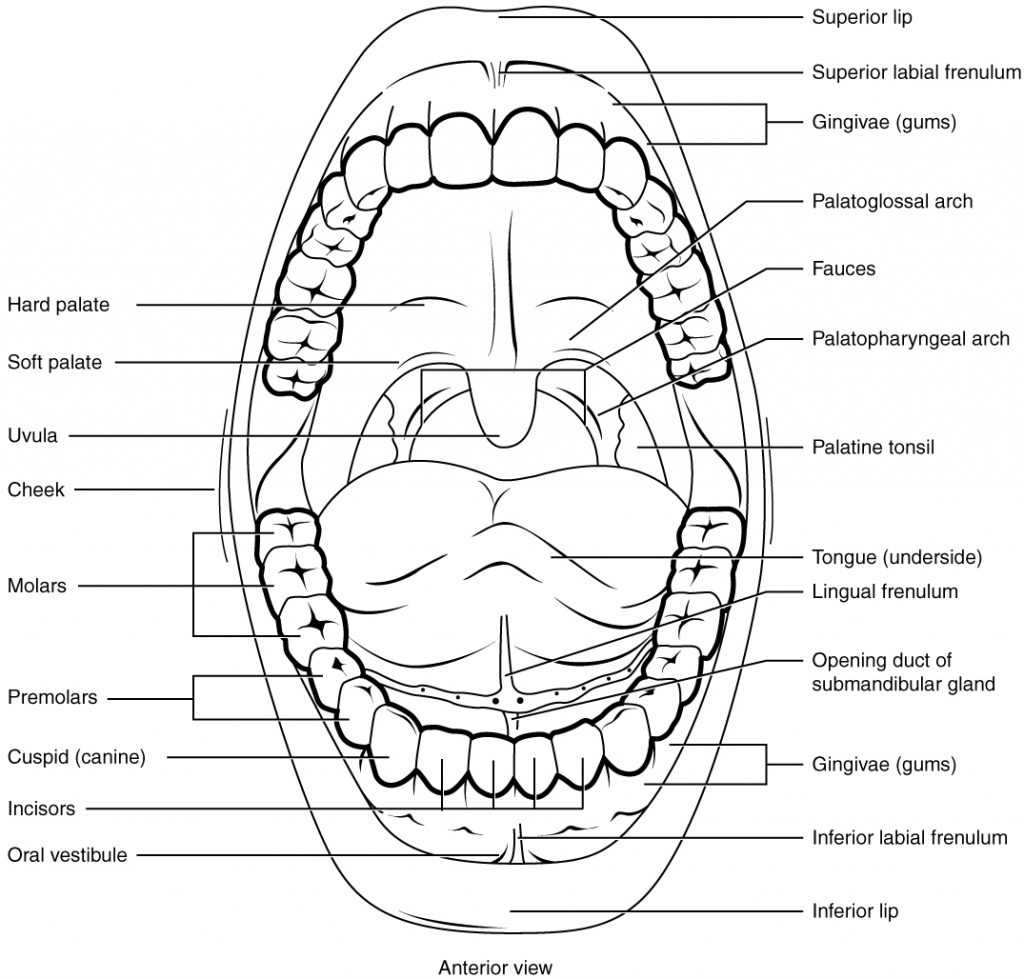
Anatomy of the Oral Cavity. (Image by OpenStax College [CC BY 3.0 , via Wikimedia Commons)
- 8 Incisors (primary aged 6 – 10 months, permanent aged 7 – 8 years)
- 4 Canine (primary aged 16 – 20 months, permanent aged 11 – 13 years)
- 8 Premolar (permanent aged 11 – 13 years)
- 12 Molar (primary aged 10 – 24 months, permanent aged 6 – 25 years)
Each tooth type is given a number starting from the front and moving backwards. So the central incisor (very front tooth) is given a number one, the lateral incisor (the next tooth along) a number 2 and so forth. The number 3 is for canines, 4,5 for premolars, and 6-8 for molar teeth. The quadrants of the mouth are marked by the two perpendicular lines, with the horizontal and vertical line showing the tooths relationship to the midline of the mouth. Sometimes teeth may be marked as being UL2 or LR3. This is a shorthand method of denoting the Upper Left 2 (UL2) or Lower right 3 (LR3).
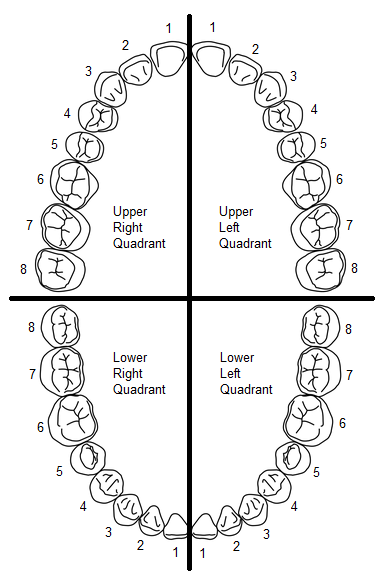
Tooth Numbering System. (Image modified by FRCEM Success. Original image [CC BY-SA 3.0 , from Wikimedia Commons)
Each tooth can be simply divided into crown and root, the clinical crown being that part of the tooth which is visible within the mouth and the root being that which is not. The majority of the crown is composed of dentine surrounded by enamel with an inner pulp chamber; the root is also composed mainly of dentine with pulp channels within. The pulp contains the neurovascular structures of the tooth, and it is here where dental pain originates.
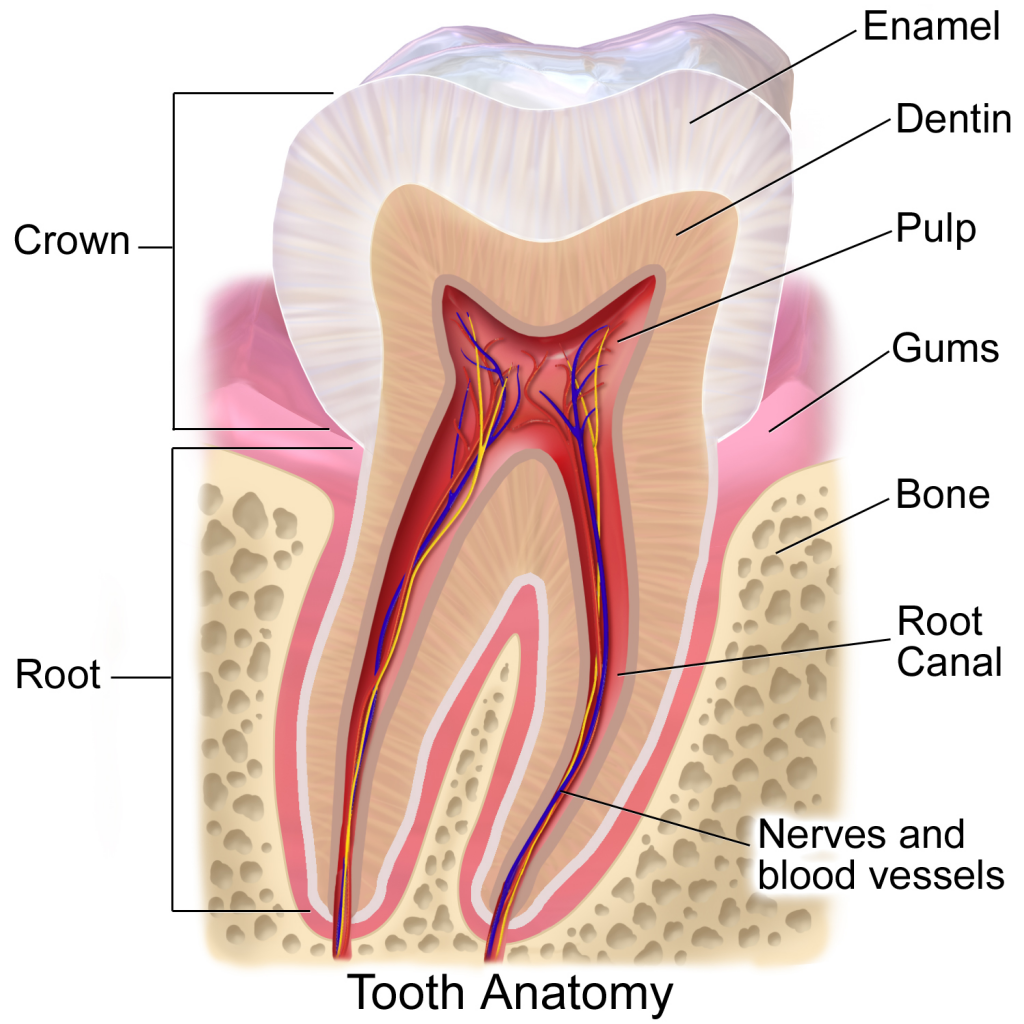
Anatomy of the Tooth. (Image modified by FRCEM Success. Original by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. (Own work) [CC BY 3.0 , via Wikimedia Commons)
Definitions
- Concussion: An injury to the tooth-supporting structures with tooth tenderness but no increase in tooth mobility, and no displacement of the tooth.
- Subluxation: An injury to the tooth-supporting structures with an increase in tooth mobility but tooth position remains correct.
- Intrusion: An injury resulting in apical displacement of the tooth (tooth is pushed into the socket).
- Extrusion: Coronal displacement of the tooth (tooth has moved out of the socket but has not come out completely).
- Lateral luxation: Movement of a tooth in any direction that isn't axial. For example, the tooth may be displaced buccally or palatally.
- Avulsion: The tooth has been completed displaced out of the socket.
- Fracture:
- Enamel fracture: Damage to the enamel of a tooth resulting in the loss of tissue, isolated to enamel only.
- Enamel and dentine fracture: Fracture of a tooth extending through both enamel and dentine, resulting in the loss of both tissues, but not extending into the dental pulp.
- Complicated crown fracture: Fracture through the tooth extending into the dental pulp of a tooth. Also known as an enamel-dentine-pulp fracture.
- Root fracture: Fracture of the apical portion of the tooth which involves dentine, pulp and cementum.
- Alveolar bone fracture: Fracture of the alveolar process of the maxilla or mandible, which may or may not involve the socket itself. Note this is not the same as a fracture to the mandible or maxilla itself, and treatment between these two conditions is different.
Assessment
- History
- Medical history including tetanus status
- Mechanism of injury
- Time of injury
- Location of missing teeth
- Any loose teeth/teeth not in the correct place
- Any new sharp edges to teeth
- If patient has missing tooth
- What medium was tooth kept in? (ideal medium is saliva or milk)
- Is the tooth an adult or baby tooth?
- Assessment
- If patient is not aware of location of missing tooth
- If there are deep lacerations in the lips or cheeks, a tooth fragment may have become lodged in these areas - a soft tissue x-ray can identify any foreign bodies
- If there is a risk that a tooth fragment may have been aspirated, a chest x-ray should be performed to exclude this
- Examine the patient for:
- Tooth avulsion
- Tooth fracture or chip
- Position of teeth (intrusion/extrusion/lateral luxation)
- Mobility of teeth (subluxation/lateral luxation)
- Signs of alveolar bone fracture (multiple blocks of teeth move when manipulating one tooth, presence of gingival tears)
- Orthopantomogram (OPG) x-ray
- Can differentiate between deciduous or adult tooth, assess degree of damage to dental and periodontal structures and differentiate between fracture at crown level and intrusion
- If patient is not aware of location of missing tooth
Management
Primary teeth:
- Treatment generally revolves around reassurance, warning patients of damage to underlying successive adult teeth (which may result in discolored, misshapen teeth).
- If the primary tooth has been avulsed then IT SHOULD NOT BE REIMPLANTED. Doing this is likely to result in further damage to the underlying adult tooth.
- If the primary teeth are very loose and present a potential airway risk, then they should be removed (which can generally be done with some local anaesthetic and a piece of gauze or a needle holder).
- An intruded primary tooth should also be considered for extraction due to the risk of damage to the underlying developing tooth germ, although this might be better performed by a general dental practitioner.
Avulsed teeth:
- The tooth should be held in a physiologically acceptable medium (saliva or milk) before re-implantation.
- It is important to hold the tooth at the crown only (the part that is normally visible in the mouth) and to avoid touching the root surface.
- Saline should be used to briefly clean debris from the root of the tooth and also to irrigate the socket to remove any blood clots that may be present here (allowing for revascularisation of the tooth).
- The tooth should be gently placed back into the socket, and splinting carried out, ensuring that the tooth is orientated correctly in the correct socket.
- Antibiotics should be given and a tetanus booster considered.
- Early and prompt referral to dental surgeon or maxillofacial surgeon is required.
- Note that in patients with immunodeficiency, it may be appropriate to avoid reimplanting the tooth due to the increased risk of infection.
- It is worth noting that teeth that are outside of the mouth for more than 60 minutes are more likely to fail and undergo root resorption (breakdown) or ankylosis (fusion of root to the bone) and ultimately fail.
Luxated, intruded and extruded teeth:
- The teeth should be replaced into the correct position, and a splint should be used to stabilise them. It is generally recommended that splinting is carried out by an individual who is dentally qualified, or has experiencing in splinting the teeth.
- The splints should remain for 2-4 weeks (this requires follow up with a dentist, who may remove the splint at 2 weeks and resplint the area).
Cracked teeth:
- Cracked teeth are more complicated to treatment plan and treat, and require assessment by a qualified dentist.
- Attempts should be made to locate missing fragments, and the patient warned about risk of future pain and requirement for future dental work.
- Sensitive toothpaste, paracetamol and NSAIDs can be recommended for these patient groups to help with pain that is likely to occur on contact with hot/cold food, drinks or other substances.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |