

Maxillofacial & Dental

A 72 year old woman presents to the Emergency Department with a 3 day history of increasing facial swelling and pain. She has a past medical history of insulin dependant diabetes. You see a periapical abscess on examination of her mouth. You decide antibiotic therapy is indicated. Which of the following antibiotics is the most appropriate first line choice?
Answer:
If an oral antibiotic is indicated prescribe a 5-day course of either amoxicillin or phenoxymethylpenicillin (clarithromycin if penicillin allergic).Dental Abscess
Maxillofacial & Dental
Last Updated: 14th December 2023
A dental abscess is a localised collection of pus in the teeth, supporting structures of the teeth (periodontal ligament, alveolar bone), or gums.
Clinical anatomy
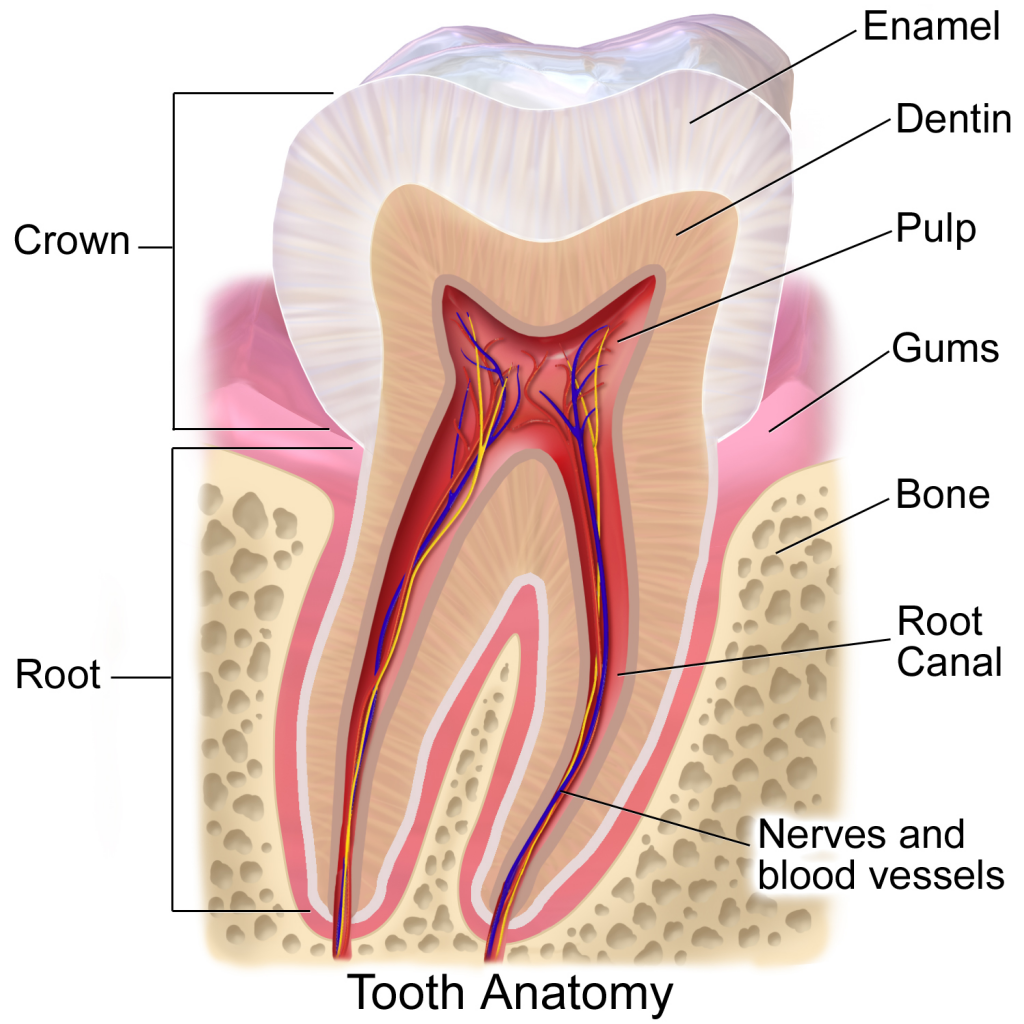
Anatomy of the Tooth. (Image modified by FRCEM Success. Original by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. (Own work) [CC BY 3.0 , via Wikimedia Commons)
Pathophysiology
Bacteria associated with dental infection include oral streptococci and anaerobes (including Prevotella, Bacteroides, and Fusobacterium species). Dental abscess is usually polymicrobial.
There are two main types of dental abscess:
- Periapical abscess — caused by infection of the root canal of the tooth usually secondary to dental caries (can also occur as a result of trauma)
- Periodontal abscess - originates in deep periodontal pockets between the tooth and the gum and occurs when there is occlusion of drainage of the periodontal pocket (as in chronic periodontitis)
Risk factors
- Poor oral hygiene
- Dental caries
- Periodontal disease
- Dental trauma
- Partially erupted or impacted tooth
- Alcohol or drug misuse
- Malnutrition
- Immunocompromise
- History of radiotherapy
- Medications causing dry mouth (for example antihistamines, anticholinergics, antidepressants)
Clinical features
- Symptoms
- Pain – usually of sudden onset, and worsens over a few hours to days, typically intense and throbbing, worse when lying down and may cause waking from sleep, pain may radiate to the ear, lower jaw and neck on the same side as the abscess
- Tooth is tender to touch, temperature or to pressure from biting
- Bad taste in the mouth
- Fever and malaise
- Trismus or dysphagia may be present in severe cases
- Listlessness, lethargy, and loss of appetite
- Signs
- Facial swelling +/- cellulitis
- Regional lymphadenopathy
- Altered tooth appearance (elevated, broken, decayed)
- Increased tooth mobility and tenderness on palpation
- Gum swelling, tenderness, warmth and purulent exudate
Management
- Ensure that the person does not have features of serious illness or complications requiring immediate treatment:
- Signs of airway compromise (for example difficulty breathing or speaking, unable to swallow their own saliva, drooling, uvular deviation, trismus, or unable to push their tongue forward out of their mouth)
- Significant systemic illness
- A rapidly progressing infection
- Significant mandibular, submandibular, or infraorbital swelling
- Floor of mouth swelling
- A spreading facial infection or orbital cellulitis
- Neurological signs (for example decreased level of consciousness, headache, eye signs [such as diplopia, papilloedema, pupil dilation, proptosis])
- Dehydration
- Emphasise the need to seek treatment from a dentist as soon as possible
- Advise that definitive treatment can only be given by a dentist and medication will not eliminate the source of infection, and that serious complications may occur if the abscess is not treated correctly by the dentist
- In absence of immediate assessment and treatment by a dentist:
- Provide appropriate self-care advice to reduce pressure and pain of the dental abscess
- Advise use of analgesic to relieve symptoms (ibuprofen, or paracetamol if ibuprofen is contraindicated or unsuitable, is recommended first-line)
- Consider the use of antibiotic treatment
- Antibiotic treatment:
- Antibiotics are generally not indicated for otherwise healthy people at low risk of complications when there are no signs of spreading infection.
- Only prescribe an antibiotic:
- For people who are systemically unwell or if there are signs of severe infection (for example fever, lymphadenopathy, cellulitis, diffuse swelling)
- For high-risk individuals to reduce the risk of complications (for example people who are immunocompromised or have diabetes)
- If an oral antibiotic is indicated prescribe a 5-day course of either amoxicillin or phenoxymethylpenicillin (metronidazole or clarithromycin if penicillin allergic)
- Consider concomitant treatment with metronidazole if the infection is severe or spreading (lymph node involvement, or systemic signs i.e. fever or malaise)
Complications
- Loss of affected tooth
- A fistula or sinus tract may develop that can discharge intraorally or into the overlying skin
- A dental cyst may develop around the apex of the tooth
- Spread of infection
- Maxillary sinusitis
- Cellulitis/periorbital cellulitis
- Osteomyelitis
- Retropharyngeal abscess
- Cavernous sinus thrombosis
- Encephalitis and meningitis
- Brain abscess
- Mediastinitis
- Ludwig's angina
- Sepsis
- Airway obstruction
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |