

Maxillofacial & Dental
A 43 year old woman presents to the Emergency Department after being punched to the right side of her face. She is complaining of trismus. X-rays have confirmed a zygomatic arch fracture. She has received intravenous morphine for analgesia and ondansetron for associated nausea. What is the most likely cause of this patient's trismus?
Answer:
The temporalis muscle and coronoid process of the mandible lie beneath the arch and may become trapped in depressed fractures of the zygomatic arch, leading to trismus.Zygomatic Arch Fracture
Maxillofacial & Dental
Last Updated: 21st March 2021
Clinical anatomy
The zygomatic arch is predominantly formed by the zygomatic process of the temporal bone which articulates with the much smaller temporal process of the zygoma forming the arch. The temporalis muscle and coronoid process of the mandible lie beneath the arch and may become trapped in depressed fractures of the zygomatic arch.
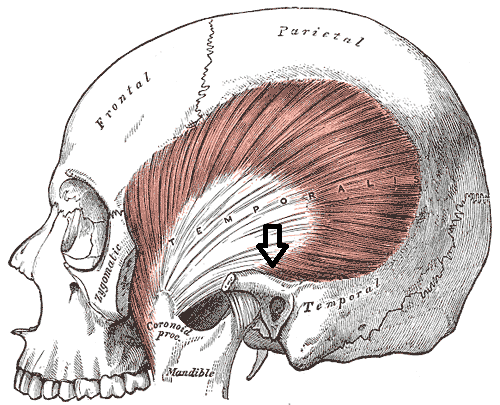
Zygomatic Arch. (Image modified by FRCEM Success. Original by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
Management
The majority of zygomatic arch fractures do not need urgent surgical intervention.
If there is restriction of mouth opening due to trapping of the temporalis muscle or coronoid process, it is an indication for urgent referral to a maxillofacial surgeon.
Discharge advice
Patients should be given general advice regarding their injury including:
- Avoidance of nose blowing as this may produce surgical emphysema
- Not to occlude the nose when sneezing
- Application of ice packs to the area to reduce swelling
- Taking regular analgesia
- General head injury advice
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |