

Maxillofacial & Dental
A 23 year old man presents to the Emergency Department complaining of pain in his jaw after being punched. Which of the following is NOT an indication to request a mandibular x-ray?
Answer:
A number of clinical findings have been identified to correlate with the presence of a mandibular fracture.| Manchester Mandibular Fracture Decision Rule | |
|---|---|
| 1. Do the patient's teeth meet abnormally (i.e. malocclusion)? | |
| 2. Is the patient unable to open his/her mouth normally (i.e. trismus)? | |
| 3. Does the patient have any broken teeth? | |
| 4. Does the patient report pain while their mouth is closed? | |
| 5. Is there a step deformity? | |
| If yes to any of the above, then request mandibular x-ray |
Mandibular Fracture
Maxillofacial & Dental
Last Updated: 14th December 2023
Fractures of the mandible are the second most common facial fracture seen in the ED after nasal fracture. Common causes include interpersonal violence (>50% of cases), falls and road traffic collisions.
Clinical anatomy
The mandible is a U shaped bone comprising two hemimandibles which are completely fused at the symphysis by the age of 2 years. The mandible articulates with the mandibular fossa of the temporal bone forming the temporomandibular joints.
The shape of the mandible, and the stability of the temporomandibular joints, leave the mandible particularly susceptible to direct lateral force. The mandible may fracture at the site of impact, but also at another point within the 'ring' of bone formed by the mandible and skull. Over half of all mandibular fractures involve more than one fracture.
The site of fracture is localised to three main areas:
- the body accounts for approximately one-third of fractures
- the condylar head and neck and coronoid process another third
- and the final third the ramus and other areas.
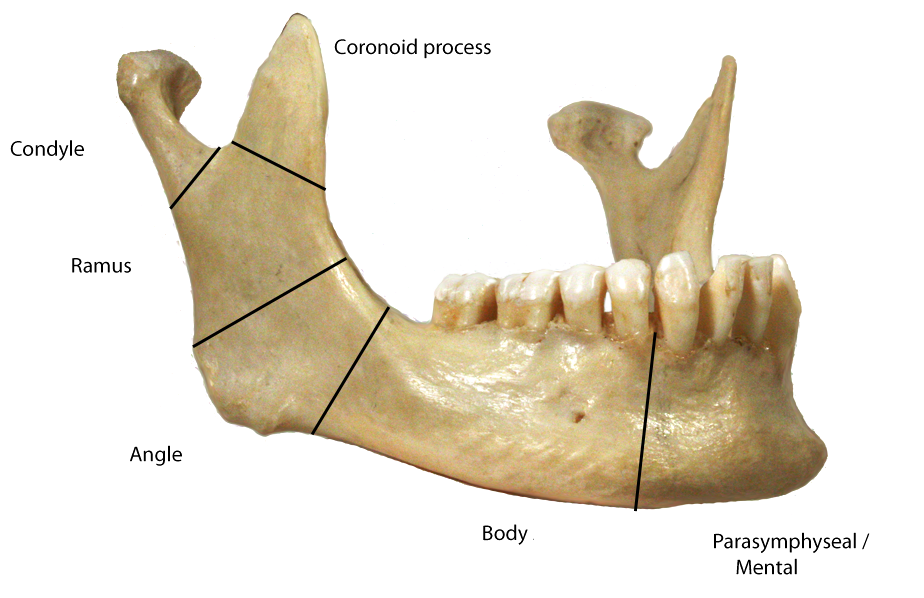
Anatomy of the Mandible. (Image by Frank Gaillard [CC BY-SA 3.0 , via Wikimedia Commons)
Risk Stratification
A number of clinical findings have been identified to correlate with the presence of a mandibular fracture.
| Manchester Mandibular Fracture Decision Rule | |
|---|---|
| 1. Do the patient's teeth meet abnormally (i.e. malocclusion)? | |
| 2. Is the patient unable to open his/her mouth normally (i.e. trismus)? | |
| 3. Does the patient have any broken teeth? | |
| 4. Does the patient report pain while their mouth is closed? | |
| 5. Is there a step deformity? | |
| If yes to any of the above, then request mandibular x-ray |
The orthopantomogram (OPG) is the most accurate technique and consequently the best initial film for screening for mandibular fracture but should be followed by additional views if clinical suspicion remains. There is greater diagnostic accuracy if the OPG is combined with an AP view of the mandible.
Helical CT scan of the mandible is an accurate method of diagnosis if x-rays are technically impossible, or CT scanning is required for other reasons.
Management
Specific management of mandibular fractures is complex and it is therefore recommended that all patients are discussed with a maxillofacial surgeon.
Factors which will influence the further management include:
- Presence of other injuries
- Location and orientation of the fracture
- Open fractures
- Potential for airway compromise
With bilateral mandibular body fractures (a flail segment) anterior tongue support is lost, resulting in posterior displacement of the tongue which occludes the airway. In this situation the patient's airway must be protected by intubation as soon as possible. As a temporary measure, ask the patient to lean forward or place them in the recovery position. If this is not possible due to other injuries, the flail segment should be grasped and pulled anteriorly, pulling the tongue forward and an oropharyngeal airway inserted.
Patients with an open mandibular fracture should be given a broad spectrum antibiotic whilst in the ED.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |