
.png)
Procedural Skills (SLO6)
You are giving a teaching session to junior colleagues regarding regional anaesthesia in the ED. You are discussing fascia iliaca blocks. Regarding fascia iliaca blocks, which of the following statements is true?
Answer:
- The landmarks for the procedure are the anterior superior iliac spine (ASIS) and the ipsilateral pubic tubercle.
- Innervation of the medial, anterior and lateral aspects of thigh comes from L2 to L4. The fascia iliaca compartment contains contains three of the four major nerves to the leg. The fascia iliaca block reliably reaches the femoral nerve and the lateral femoral cutaneous nerve. The obturator nerve is not reliably blocked.
- With a sharp needle the sensation of a “pop” when perforating a fascial layer would not be perceived.
- Overall a fascia iliaca block has a very low risk profile. The location of the injection means the risk of intravascular injection, local anaesthetic toxicity, and mechanical nerve damage is extremely low.
- The fascia iliaca compartment is a potential space in the inguinal region bordered anteriorly by the posterior surface of the fascia iliaca and posteriorly by the anterior surface of the iliacus muscle and the psoas major muscle.
Fascia Iliaca Block
Procedural Skills (SLO6)
Last Updated: 28th February 2022
Fascia Iliaca Block (FIB) should be available in Emergency Departments as part of the pain management strategy for patients with fractured neck of femur.
Advantages
The fascia iliaca compartment block performed by landmark technique is inexpensive, safe and easy to perform. It delivers effective pain relief whilst avoiding the undesirable side effects of certain other forms of analgesia. Delivering large volumes of low concentration local anaesthetic helps to maximise the benefits of the block, whilst following the well-established techniques help to minimise complications.
The advantages of FIB over Femoral Nerve Block (FNB) are:
- Lower risk of intraneural and intravascular injection
- Additional blockade of lateral femoral cutaneous nerve
- Can be performed landmark guided rather than ultrasound guided safely
Relevant anatomy
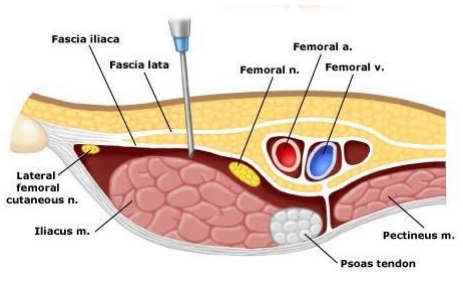
The fascia iliaca compartment is a potential space in the inguinal region bordered anteriorly by the posterior surface of the fascia iliaca and posteriorly by the anterior surface of the iliacus muscle and the psoas major muscle. FIB allows deposition of local anaesthetic of sufficient volumes to spread to at least two of the three major nerves that supply the medial, anterior and lateral thigh with one simple injection, namely the femoral and lateral femoral cutaneous nerves.
The landmarks for the procedure are the anterior superior iliac spine (ASIS) and the ipsilateral pubic tubercle. Place one finger on each of these bony landmarks and draw an imaginary line between them. Using your index fingers divide this line into thirds. At the junction of the lateral 1/3 and medial 2/3 make a mark. Your insertion point will be 1 cm inferior to this mark.
Fascia Iliaca Block
Contraindications
- Patient refuses procedure
- Allergy or intolerance to local anaesthetic
- Coagulopathy
- Infection at injection site
- Patient unable to report possible toxicity e.g. dementia, obtunded
- Inability to identify landmarks
- Previous femoral vascular surgery
Procedure
- Obtain consent
- Prepare equipment and drugs
- For skin infiltration: e.g. 1 - 2 ml of 1% lignocaine
- For FIB: 30 - 40 ml of long acting local anaesthetic (LA) e.g. 0.25% (2.5 mg/ml) chirocaine/levobupivacaine, 30 ml if patient weighs < 50 kg or 40 ml if patient weighs > 50 kg
- Position patient in supine position
- Ensure patient has IV access and resuscitation equipment is nearby
- Ensure patient is monitored (3-lead ECG, NIBP, SpO2, RR, GCS)
- Find line joining anterior superior iliac spine (ASIS) and pubic tubercle
- Find and mark junction where lateral one-third and medial two-thirds meet and move inferiorly 1 cm from this point
- Palpate to ensure you are not close to femoral artery (this should be palpable approx. 1.5 - 2 cm medial to the intended injection site); if you are, recheck landmarks and if still over artery, abandon procedure
- Skin prep, sterile gloves, drape area
- Raise small bleb of LA at intended skin puncture site
- Pierce skin with a large gauge needle at right angles to its surface
- Change to blunt ended needle connected via short extension tube to syringe of LA
- Advance needle (aspirating every 5 ml) perpendicular to skin, and feel for two 'pops' indicating you have crossed the fascia lata, followed by the fascia iliaca
- Advance the needle a further 1 - 2 mm
- Aspirate again, and then slowly inject LA while asking patient how they feel throughout, being vigilant for signs of LA toxicity or accidental injection into a nerve (severe pain or paraesthesia); stop injection if adverse effects occur (there should be no resistance to injection, if there is, the needle is likely to be in the iliacus muscle; in this case withdraw the needle slightly until injection is easy)
- After injection, withdraw needle and apply 30 secs - 2 mins of pressure distal to injection site to direct LA proximally
- Dress injection site
- Ensure patient is comfortable and that observations are checked:
- Every 5 minutes for 15 minutes
- At 30 minutes
- 4-hourly thereafter
- If no pain relief after 30 minutes, offer alternate analgesia; do not repeat block
Complications
- Failure of technique to provide analgesia
- Trauma to closely associated structures
- Intravascular injection
- Temporary or permanent nerve damage
- Infection
- Bleeding
- Local anaesthetic toxicity
- Risks reduced by dose reduction in patients with lower body weight, aspiration every 5 ml, close monitoring of patients during and after procedure, avoidance of procedure in those who cannot report early signs of toxicity e.g. obtunded patients
- Allergy to any of the preparations used
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |