
.png)
Procedural Skills (SLO6)
A 72 year old man presents to ED complaining of abdominal pain radiating to his back which came on about 4 hours ago. You ask your consultant to perform an abdominal aorta ultrasound. Regarding abdominal aorta ultrasound, which of the following statements is true?
Answer:
- Approximately 90 - 95% of abdominal aortic aneurysms (AAA) are confined to the infrarenal aorta.
- In the acute setting, an AAA is defined as a transverse aortic diameter greater than 3 cm.
- The maximum external diameter of the aorta should be measured (measured from outer wall to outer wall).
- The aorta is situated anterior to the vertebral bodies and left of the midline, whereas the IVC lies to the right of the midline. The aorta tapers and tends to be tortuous and move to the left. It can be calcified anteriorly which can made the ultrasound view more difficult.
- Fusiform aneurysms are the type most commonly seen in the abdominal aorta. Most fusiform aneurysms are true aneurysms. The weakness is often along an extended section of the aorta and involves the entire circumference of the aorta. The weakened portion appears as a roughly symmetrical bulge.
Abdominal Aorta Ultrasound
Procedural Skills (SLO6)
Last Updated: 16th July 2025
Indications for abdominal aorta ultrasound
Features of a suspected abdominal aortic aneurysm (AAA) include:
- Unexplained back or abdominal pain in an older patient
- Renal colic in an older patient
- Syncopal episode in an older patient
- Clinical examination
- Risk factors:
- Ischaemic heart disease
- Peripheral vascular disease
- Age
Computed tomography (CT) is the gold standard investigation for suspected abdominal aortic aneurysm, but can lead to a delay in definite diagnosis and treatment. An early ultrasound is the primary investigation of choice. The combination of an aneurysm on ultrasound, together with an unstable or symptomatic patient, is enough to warrant an emergency vascular surgery opinion.
In the emergency setting it is usually difficult to define the limits or relations of the aneurysm. Likewise, ultrasound is not accurate in determining the presence of a leak from the aneurysm. Emergency Medicine AAA assessment is a focused examination to answer a single clinical question: Is an abdominal aortic aneurysm (with a diameter of greater than 3cm) present?
Clinical anatomy
Approximately 90 - 95% of abdominal aortic aneurysms (AAA) are confined to the infrarenal aorta. In the acute setting, an AAA is defined as a transverse aortic diameter greater than 3 cm.
Before starting to scan the aorta, it is helpful to understand the anatomy.
- The coeliac axis is 1-2 cm below the diaphragm.
- The superior mesenteric artery is 2 cm below the coeliac axis.
- The inferior mesenteric artery is 4 cm above the bifurcation.
- The aorta bifurcates at or immediately below the the umbilicus (L4).
- The maximum external diameter (measured from outer wall to outer walls) at different levels will vary i.e. 3 cm at the epigastrium, 1.5 cm at the bifurcation.
Aneurysms
- Fusiform aneurysms are the type most commonly seen in the abdominal aorta. Most fusiform aneurysms are true aneurysms. The weakness is often along an extended section of the aorta and involves the entire circumference of the aorta. The weakened portion appears as a roughly symmetrical bulge.
- Saccular aneurysms appear like a small blister or bleb on the side of the aorta and are asymmetrical. They may be be pseudoaneurysms caused by trauma, or by a penetrating aortic ulcer.
- Dissection aneurysms occur when a tear begins within the wall of the aorta causing the wall layers to separate. Dissections can cause aneurysms, but an existing aneurysm can also dissect. This is more commonly seen in the thoracic aorta.
Understanding the ultrasound
- The inferior vena cava (IVC) and aorta are both seen in most cases. It is possible for a novice for confuse the two.
- The aorta is situated anterior to the vertebral bodies and left of the midline, whereas the IVC lies to the right of the midline. The aorta tapers and tends to be tortuous and move to the left. It can be calcified anteriorly which can made the ultrasound view more difficult.
- The main features of the IVC are:
- Right side
- Thin walled
- Compressible
- Transmitted pulse ('double bounce')
- Almond shaped - shape varies
- The main features of the aorta are:
- Left side
- Thick walled
- Will not compress
- Pulsatile
- Round in shape - shape constant
- Superior mesenteric artery (SMA) demonstrated
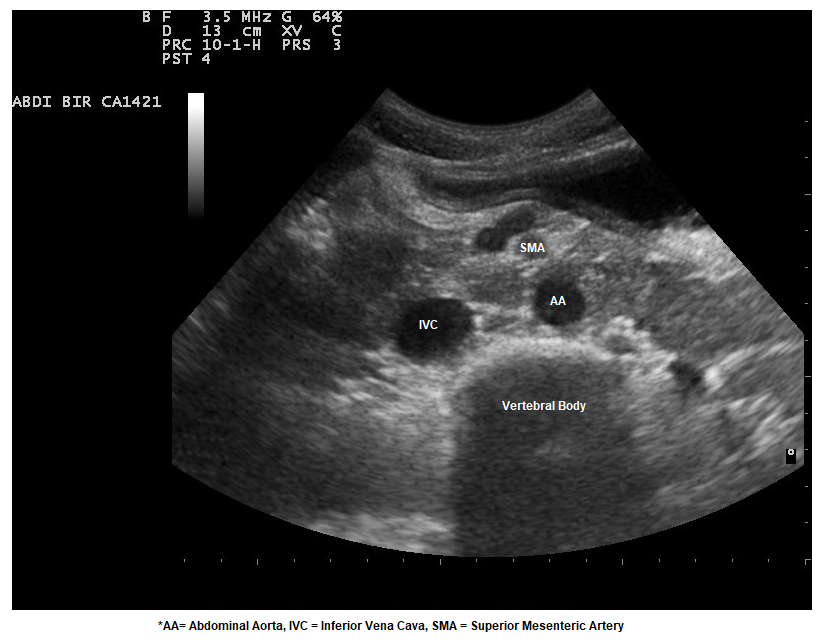
Aorta Ultrasound (Transverse View). (Image Modified by FRCEM Success. Original image by © Nevit Dilmen / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0))
Performing the ultrasound
- Start at the epigastrium. Aim to get as high as you can for the first view. If the patient has eaten recently it may not be possible to view beyond the stomach/duodenum. Firstly, begin with the patient in the supine position.
- Start with a transverse section. You should image the coeliac axis, then the superior mesenteric artery. Lower you will find the renal vessels, and around the umbilicus, the bifurcation and origin of the iliac arteries. The coeliac axis is seen high in the epigastrium. The division into splenic artery and hepatic artery is said to resemble the wings of a seagull. Often bowel gas obscures the coeliac axis and this view may be difficult to obtain. Lower down is the superior mesenteric artery which has a characteristic appearance. Identify the vertebral body (pre-vertebral stripe and acoustic shadow). The aorta lies anterior to the echo-bright pre-vertebral stripe. Use the left lobe of the liver as the initial acoustic window.
- Secondly obtain longitudinal images of the entire abdominal aorta. The aorta moves from quite deep at the diaphragm to much more shallow at the umbilicus - this is due to normal lumbar lordosis.
- Thirdly, move the probe slightly over to the right to view the inferior vena cava in longitudinal section.
- Viewing the IVC as it passes through the diaphragm can give an indication of the load on the right side of the heart.
- In unventilated patients, if the IVC diameter is > 25 mm with minimal collapse, this is indicative of increased right atrial pressure e.g. cor pulmonale, fluid overload. A diameter of < 15 mm with complete collapse is indicative of being underfilled, and a useful indicator of hypovolaemic shock.
- In ventilated patients , the correlation between IVC diameter and right atrial pressure is less reliable.
- Finally measure the anteroposterior diameter of the aorta (in the transverse view). The measurement should be from outer wall to outer wall of the vessel. Any clot or false lumen should be ignored when measuring.
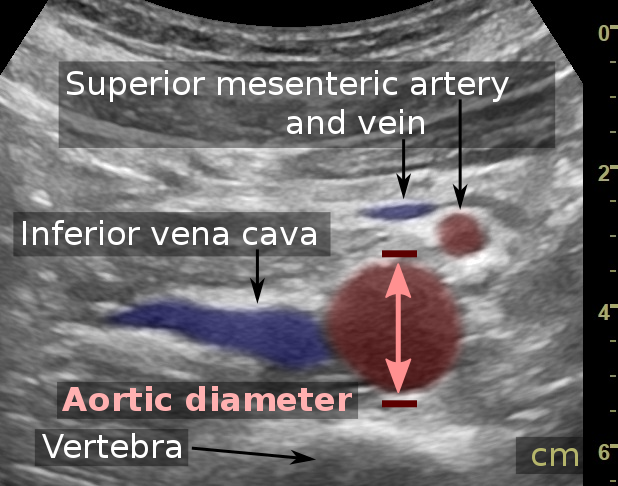
Aortic Ultrasound. (Mikael Häggström, M.D. Written informed consent was obtained from the individual, including online publication. / CC0)
Pitfalls
- Taking a non-perpendicular view of the vessel, thereby creating a 'salami slice' , with over-estimation of the diameter. As the aorta is angled against the lumbar lordosis, the probe often needs to point slightly caudally to overcome this.
- Failing to appreciate a tortuous aorta, although this is only cause significantly problems with transverse measurements.
- Not recognising the presence of a clot within the lumen leading to potential under-estimation of the diameter.
- Excluding a AAA without visualising the whole abdominal aorta and proximal iliac arteries.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |