

Ophthalmology
A 32 year old man presents to the Emergency Department with a painful, red eye. He tells you he noticed an insect bite to the face 2 days ago. You suspect periorbital cellulitis. Which of the following signs does NOT differentiate orbital from periorbital cellulitis?
Answer:
Clinical features of periorbital and orbital cellulitis- Symptoms
- Both
- A history of recent sinus infection or eyelid injury
- Redness, swelling and tenderness of eye
- Fever and systemic symptoms e.g. malaise (should raise suspicion of orbital cellulitis)
- Orbital cellulitis
- Headache
- Pain with eye movements
- Visual loss
- Diplopia
- Both
- Signs
- Both
- Visible orbital trauma, insect bite, stye or chalazion
- Eyelid oedema and erythema
- Tenderness around eye
- Orbital cellulitis
- Reduced visual acuity
- Proptosis
- Chemosis (conjunctival swelling)
- Ophthalmoplegia with diplopia
- Afferent pupillary defect
- Both
Periorbital and Orbital Cellulitis
Ophthalmology
Last Updated: 8th September 2021
Clinical anatomy
The orbital septum is a thin sheet of fibrous tissue that originates from the orbital rim periosteum and blends with the tendon of the levator palpebrae superioris superiorly and inserts into the tarsal plate inferiorly. It effectively separates the eyelids from the contents of the orbital cavity.
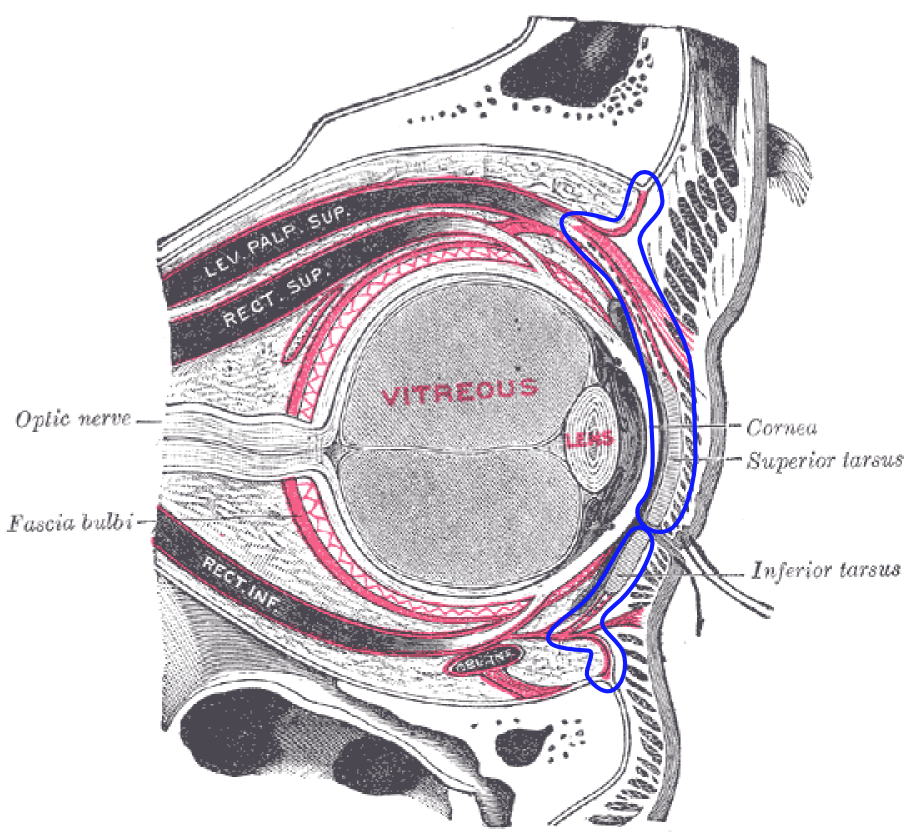
Orbital Septum. (Image by Mikael Häggström, used with permission. (File:Gray891.png) [Public domain])
Definition
Periorbital cellulitis is an infectious process occurring in the eyelid tissues superficial to (anterior to or above) the orbital septum. Periorbital cellulitis is of concern in children because it may rapidly progress to orbital cellulitis.
Orbital cellulitis is an infectious process affecting the muscles and fat within the orbit, posterior or deep to the orbital septum. Orbital cellulitis has much higher morbidity than periorbital cellulitis, and warrants urgent imaging and surgical evaluation.
Aetiology
Periorbital cellulitis is usually due to superficial tissue injury (e.g. insect bite, stye, chalazion) but may be secondary to bacterial sinusitis in children.
Orbital cellulitis is usually due to underlying bacterial sinusitis or another upper respiratory tract infection. Less common sources of orbital cellulitis are orbital injury, fracture, dacryocystitis, endophthalmitis or underlying dental infections. More rarely, infection may spread haematogenously.
Organisms involved include Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus species, and anaerobes. In immunised adults and children, Haemophilus influenzae is essentially no longer a concern.
Clinical features
- Symptoms
- Both
- A history of recent sinus infection or eyelid injury
- Redness, swelling and tenderness of eye
- Fever and systemic symptoms e.g. malaise (should raise suspicion of orbital cellulitis)
- Orbital cellulitis
- Headache
- Pain with eye movements
- Visual loss
- Diplopia
- Both
- Signs
- Both
- Visible orbital trauma, insect bite, stye or chalazion
- Eyelid oedema and erythema
- Tenderness around eye
- Orbital cellulitis
- Reduced visual acuity
- Proptosis
- Chemosis (conjunctival swelling)
- Ophthalmoplegia with diplopia
- Afferent pupillary defect
- Both
Investigation
- First Choice
- CT sinus and orbits with contrast (for suspected orbital cellulitis)
- WBC count (usually raised)
- To Consider
- Blood cultures (often negative)
- Swabs (from conjunctiva, nasopharynx or external wounds as necessary)
- MRI head and orbits with contrast (for patients demonstrating neurological deficit)
- Lumbar puncture (for patients with meningeal signs)
Management
- Empirical broad-spectrum antibiotics initially, with therapy targeted according to cultures if positive
- Periorbital cellulitis:
- The majority of paediatric cases require immediate empirical intravenous antibiotic therapy. Alternatively, empirical oral therapy may be initiated in children with reliable daily follow-up.
- In adults who are adherent and stable, oral antibiotics should be administered with careful follow-up.
- Clinical improvement is usually seen within 24 to 48 hours. Prognosis is excellent, with full resolution in almost all cases. Progression to orbital cellulitis in immunocompetent adults with no underlying risk factor is rare.
- Orbital cellulitis:
- All patients with orbital cellulitis should be admitted for empirical intravenous antibiotic therapy.
- Prompt orbital imaging for underlying sinusitis/orbital abscess is mandatory; patients may require surgical drainage.
- A lag time of 24 to 48 hours commonly occurs between initiation of antibiotics and clinical response. If there is no improvement or if new signs such as decreased vision or afferent pupillary defect appear, repeat CT scan and suspect abscess formation or resistant organisms.
- Periorbital cellulitis:
Complications
- Subperiosteal abscess
- Ocular empyema
- Orbital abscess
- Ocular compartment syndrome
- Permanent vision loss
- Retinal artery occlusion
- Meningitis
- Epidural or brain abscess
- Cavernous sinus thrombosis
Comparison of periorbital and orbital cellulitis
| Orbital cellulitis | Periorbital cellulitis |
|---|---|
| Definition: Infectious process affecting the muscles and fat within the orbit, posterior or deep to the orbital septum | Definition: Infectious process occurring in the eyelid tissues, superficial to (anterior to or above) the orbital septum |
| Aetiology: Most commonly secondary to underlying bacterial sinusitis | Aetiology: Most commonly secondary to superficial eyelid injury e.g. insect bite, chalazion |
| Clinical features: Red tender swollen eye, pain with eye movements, visual loss, proptosis, chemosis, ophthalmoplegia and diplopia, afferent pupillary defect, headache, fever, malaise | Clinical features: Red tender swollen eye |
| Management: Immediate admission and ophthalmology involvement, empirical intravenous broad spectrum antibiotic therapy, CT imaging of orbit and sinuses, surgical evaluation | Management: Empirical broad spectrum antibiotic therapy; adults can usually be managed with oral antibiotics and careful follow-up, children are usually admitted for intravenous antibiotics |
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |