

Sexual Health
This was previously featured in an exam
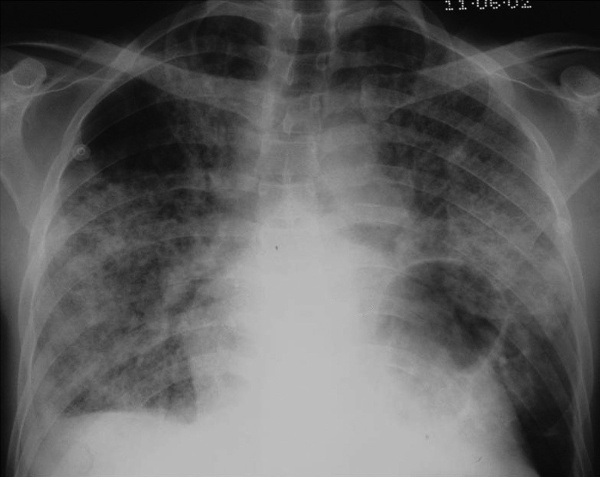
A 45 year old man, with a known history of HIV, presents to ED complaining of a 2 week history of a worsening dry cough and breathlessness. What is the most likely diagnosis?
Answer:
The x-ray shows patchy ground glass opacities and a pulmonary cyst, which together with the history of HIV, make the diagnosis most likely Pneumocystis pneumonia. Pneumocystis pneumonia (PCP) is an infection of the lung caused by the fungal organism Pneumocystis jirovecii (formerly known as Pneumocystis carinii). Suspicion for PCP is based on clinical signs or symptoms of pneumonia in a person with immune suppression, especially when due to HIV infection. The cough is typically dry/non-productive because sputum becomes too viscous to be coughed up. The dry cough distinguishes PCP from typical pneumonia. Diagnosis is made by detection of the organism in either induced sputum or bronchoalveolar lavage. Blood gas measurement is used to assess disease severity. The treatment of choice is trimethoprim/sulfamethoxazole (TMP/SMX).Human Immunodeficiency Virus
Infectious Diseases / Sexual Health
Last Updated: 6th March 2026
HIV (human immunodeficiency virus) is a lentivirus from the retrovirus subfamily. Lentiviruses have a long latent phase between infection and the development of symptoms.
There are 2 main types of HIV — HIV-1 and HIV-2.
- HIV-1 is highly virulent and is found worldwide.
- HIV-2 is found mainly in West Africa but has also been reported in Portugal, France, and increasingly in India and South America.
HIV causes immunodeficiency by preferentially infecting and destroying cells of the immune system, in particular the CD4 cells, a class of T lymphocytes which are also known as T helper cells.
Stages of Infection
- Primary HIV infection/HIV seroconversion illness
- Early phase, occurring about 2-4 weeks after infection.
- During this stage, some people develop flu-like symptoms, such as fever, sore throat, rash, swollen lymph nodes, and fatigue, while others remain asymptomatic.
- The virus multiplies rapidly and spreads throughout the body, attacking and destroying the CD4 cells.
- The viral load is very high in this phase; the person affected is highly infectious.
- Asymptomatic phase
- Follows resolution of the primary infection and may persist for several years.
- Most people remain well, although HIV continues to replicate at low levels, gradually weakening the immune system as CD4 cells decline.
- The person remains infectious despite the absence of symptoms.
- Symptomatic phase
- Develops as immune function further declines.
- HIV-related complications emerge, including minor opportunistic infections (such as oral thrush or shingles) and multisystem complications (such as respiratory, neuropsychiatric, metabolic, dermatological, and renal problems).
- These complications result from chronic HIV infection, persistent immune activation, treatment effects, co-infections, comorbidities, and/or lifestyle factors.
- Symptoms may resolve with treatment but can recur or evolve, and new problems may arise at later stages.
- Advanced HIV disease (AIDS [acquired immunodeficiency syndrome])
- Occurs when the immune system is severely weakened.
- Defined by a CD4 cell count below 200 cells per microlitre or the occurrence of certain opportunistic infections (such as Pneumocystis pneumonia) or malignancies (such as Kaposi’s sarcoma), collectively known as AIDS-defining conditions.
Transmission
In a person infected with HIV, the virus is present in cell-containing bodily fluids, such as blood, semen, vaginal secretions, breast milk, amniotic fluid, pleural effusions, and cerebrospinal fluid.
Infected bodily fluid can transmit HIV:
- Sexual activity (vaginal, anal, or oral sex, especially in the presence of oral disease, such as ulceration or gingivitis).
- Vertically from mother to child (during pregnancy, childbirth, or breastfeeding).
- By inoculation (via contaminated needles, instruments, blood, or blood products; through direct exposure of mucous membranes or an open wound to infected bodily fluids; or by a human bite that breaks the skin).
In the UK, HIV infection is most prevalent among men who have sex with men and black-African heterosexual men and women. In the UK, the number of HIV infections acquired through injecting drug use and mother-to-child vertical transmission is low.
Risk factors
Risk factors for HIV infection include:
- Sexual behaviour:
- Unprotected sex.
- Multiple sexual partners.
- High-risk sexual practices (such as chemsex).
- Specific populations:
- Men who have sex with men (MSM).
- Trans women
- Trans men with additional risk factors (such as receptive sex with partners living with HIV).
- People who inject drugs.
- Sex workers
- Black Africans.
- People in prisons or other closed settings.
- People from a country with a high diagnosed seroprevalence (more than 1%).
- Exposure through partners or family:
- Female partners of MSM.
- Sexual partners of people living with HIV.
- Sexual partners of people from high HIV prevalence countries.
- People with a mother living with HIV.
- Other exposures:
- History of other sexually transmitted infections (such as syphilis, chlamydia, and gonorrhoea).
- Blood transfusions, transplants, or other invasive procedures in countries without rigorous HIV screening.
- Occupational exposure (for example, sharps and mucosal splash injuries).
- Sexual assault or rape.
Prognosis
Advances in antiretroviral therapy (ART) have transformed HIV infection into a manageable chronic disease. Prompt initiation of ART preserves CD4 cell counts and markedly reduces the risk of developing advanced HIV disease. With timely diagnosis and lifelong adherence to ART, people living with HIV can now expect a near-normal life expectancy. Those who maintain an undetectable viral load on ART cannot transmit the virus sexually. This approach, known as treatment as prevention (TasP), underpins the public health message 'Undetectable=Untransmittable' (U=U).
Untreated HIV or ART failure leads to advanced HIV disease, defined by opportunistic infections (such as Pneumocystis pneumonia) or malignancies (such as Kaposi’s sarcoma), collectively known as AIDS-defining conditions. Even with effective ART, people with long-standing HIV may develop complications due to chronic infection, immune activation, treatment effects, co-infections, comorbidities, and/or lifestyle factors.
HIV Indicator Conditions
HIV indicator conditions are health problems that should prompt consideration of an HIV test because they indicate a higher likelihood of HIV infection. They are divided into the following categories:
- Category 1 - Potentially AIDS defining conditions (which strongly suggest advanced HIV infection or AIDS).
- Category 2a - Conditions in which the prevalence of undiagnosed HIV is more than 0.1%.
- Category 2b - Conditions likely to have an undiagnosed prevalence of HIV of more than 0.1%.
- Category 3 - Conditions likely to have an estimated prevalence of HIV lower than 0.1% but where not identifying HIV infection may have significant adverse implications for the person's care.
Category 1 (potentially AIDS defining conditions) includes:
- Cancers
- Cervical cancer
- Non-Hodgkin's lymphoma
- Kaposi's sarcoma
- Bacterial infections
- Mycobacterium tuberculosis (pulmonary or extrapulmonary)
- Mycobacterium avium complex or Mycobacterium kansasii (disseminated or extrapulmonary)
- Other or unidentified Mycobacterium species (disseminated or extrapulmonary)
- Recurrent pneumonia (2 or more episodes in 12 months)
- Recurrent Salmonella septicaemia
- Viral infections
- Cytomegalovirus (CMV) retinitis
- Other CMV infections (except liver, spleen, glands)
- Herpes simplex virus: ulcer(s) for more than 1 month, bronchitis, or pneumonitis
- Progressive multifocal leukoencephalopathy
- Parasitic infections
- Cerebral toxoplasmosis
- Cryptosporidiosis diarrhoea for more than 1 month
- Isosporiasis for more than 1 month
- Atypical disseminated leishmaniasis
- Reactivation of American trypanosomiasis (meningoencephalitis or myocarditis)
- Fungal infections
- Pneumocystis jirovecii (previously P. carinii) pneumonia (PCP)
- Oesophageal candidiasis
- Candidiasis of bronchial/tracheal/lung sites
- Extrapulmonary cryptococcosis
- Disseminated/extrapulmonary histoplasmosis
- Disseminated/extrapulmonary coccidioidomycosis
- Disseminated penicilliosis
HIV Testing
If HIV testing is indicated, appropriate information should be provided to ensure that the person can access testing in a way that meets their needs and preferences. The need for repeat testing should be considered.
The diagnostic tests currently used for the diagnosis of HIV infection are:
- Third-generation tests, which detect HIV antibodies (IgM and IgG) only.
- Fourth-generation tests, which detect both HIV antibodies (IgM and IgG) and p24 antigen.
The choice of test depends on the urgency of results, the availability of testing methods, and the person's preference.
- The recommended first-line test is fourth-generation laboratory testing of venous blood.
- If rapid results are needed, Point-of-care tests (POCTs) can be performed.
- For people who decline venous blood testing, decline an immediate offer of a test, or prefer to test outside a clinical setting, self-testing and self-sampling kits are available.
The window period of HIV is defined as the time interval between exposure to infection and accurate detection of that infection.
Window periods are:
- For fourth-generation laboratory tests - 45 days.
- For third-generation laboratory tests - 60 days.
- For all POCTS - 90 days.
Tests may be performed early within the window period, but if the initial test is negative, a repeat test should be offered at the appropriate interval after potential HIV exposure.
Management
The role of the HIV clinic includes to:
- Initiate and monitor antiretroviral therapy (ART).
- Conduct necessary monitoring, including CD4 counts and viral load, routine blood tests, and screening for other sexually transmitted infections (STIs).
- Provide preventive care, including cardiovascular disease (CVD) risk assessment and management and cervical smears (for women).
- Manage complications and comorbidities, including opportunistic infections, multisystem complications, and mental and sexual health problems.
- Offer counselling and support.
Antiretroviral Therapy
Antiretroviral therapy (ART) has had a huge positive impact on HIV-related morbidity and mortality and aims to reduce viral load to undetectable levels by limiting viral replication. HIV mutates as it replicates, so ART is usually used in combinations of three or more to reduce drug resistance. Specialist blood tests may be used to identify drug resistance and tailor ART regimens accordingly. ART suppresses viral replication but does not eliminate HIV; therefore, treatment is lifelong.
There are five main classes of antiretroviral drugs, which work at different stages of the HIV lifecycle:
- Nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), such as zidovudine and lamivudine, mimic the building blocks of DNA. When incorporated into viral DNA by HIV reverse transcriptase, an enzyme that converts viral RNA into DNA, they cause premature chain termination, preventing viral replication.
- Non-nucleoside reverse transcriptase inhibitors (NNRTIs), such as efavirenz and nevirapine, bind directly to HIV reverse transcriptase, altering its shape. This prevents the enzyme from converting viral RNA into DNA, thereby halting viral replication.
- Protease inhibitors (PIs), such as darunavir and atazanavir, block HIV protease, an enzyme that cleaves viral polyproteins into functional proteins. Without this step, newly formed virions cannot mature properly and remain non-infectious.
- Integrase Inhibitors (INSTIs), such as dolutegravir and raltegravir, inhibit HIV integrase, the enzyme responsible for integrating viral DNA into the host genome. By blocking this step, they prevent the virus from establishing an infection in host cells.
- Entry Inhibitors (EIs), such as maraviroc and enfuvirtide, prevent HIV from entering host cells. Maraviroc blocks the CCR5 co-receptor, a protein that HIV uses to attach to immune cells, while enfuvirtide inhibits fusion of the viral and cell membranes, stopping viral entry.
ART can cause a range of adverse effects, some of which may be serious or life-threatening. While older drug classes carry the highest risk, all antiretrovirals have potential short- and long-term toxicities. Adverse effects include:
- Hypersensitivity reactions — typically cause fever or rash, but can cause non-specific symptoms, such as fever, vomiting, or myalgia. These reactions can be life-threatening, so specialist advice should be sought if suspected.
- Neurological and psychiatric conditions — nightmares, sleep disturbance, mood or behaviour changes may occur; psychosis and suicidal ideation have also been reported.
- Hyperlipidaemia (common) — rises in cholesterol or triglycerides can be extreme, and lipids need to be regularly monitored and managed. Drug interactions with statins and fibrates occur frequently and can be serious. Seek specialist advice before prescribing.
- Lipodystrophy (changes in the distribution of body fat) and lipoatrophy (loss of subcutaneous fat) — these may be associated with diabetes and hyperlipidaemia.
- Type 2 diabetes mellitus — most likely occurs through insulin resistance and can be associated with ART.
- Bone density loss — people with HIV are at higher risk of osteopenia, osteoporosis, and fractures, likely due to a combination of factors such as ART, lifestyle, and previous steroid treatment.
- Renal problems — a decline in renal function may indicate Fanconi’s syndrome (dysfunction of the proximal tubule); specialist advice should be sought. Ureteric colic, renal and ureteric stones may also occur.
- Lactic acidosis and hepatic toxicity — may present with non-specific symptoms, such as nausea, anorexia, or abdominal pain, and are potentially life-threatening.
- Peripheral neuropathy.
- Bone marrow suppression.
- Pancreatitis (most often associated with older ART).
Monitoring
Monitoring of HIV is typically conducted in specialist clinics using the CD4 lymphocyte (CD4) count and viral load.
The CD4 count reflects the degree of immunosuppression in people with HIV:
- In a healthy person not infected with HIV, the CD4 count is usually greater than 500 cells per microlitre; some people may have naturally lower counts.
- People with CD4 counts below 200 cells per microlitre are most at risk of HIV-related opportunistic infections and cancers.
- If treatment is started at CD4 counts above 500 cells per microlitre, rather than later, prognosis is improved.
Viral load reflects rates of viral replication and is measured using a polymerase chain reaction (PCR) test:
- A rising viral load may indicate non-adherence to antiretroviral therapy (ART), resistance to one or more antiretroviral drugs, or an interaction with another medication.
- Viral load ranges from undetectable (less than 20–50 copies of viral genome/mL blood) to over a million copies/mL.
- The degree of viral replication is linked to the rate of CD4 decline and, therefore, disease progression. When viral load is suppressed through ART, CD4 counts recover, and the risk of HIV-related complications declines.
Prevention
Pre-exposure prophylaxis
Pre-exposure prophylaxis (PrEP) is usually a combination of two antiretroviral drugs taken to reduce the risk of HIV acquisition before potential exposure. It should be started as soon as HIV risk is identified. The benefits are immediate, and toxicity is uncommon.
PrEP is not indicated for people who only have sex with HIV-positive partner(s) on antiretroviral therapy (ART) with a viral load less than 200 copies/mL, as the risk of HIV transmission is zero.
Post-exposure prophylaxis
Post-exposure prophylaxis (PEP) is a 28-day course of antiretroviral therapy (ART) that reduces the risk of HIV infection following a recent potential exposure. It should be initiated as soon as possible, ideally within 24 hours and no later than 72 hours post-exposure. Efficacy decreases with delay, and tolerability is generally good.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |