

Surgical Emergencies
This was previously featured in an exam
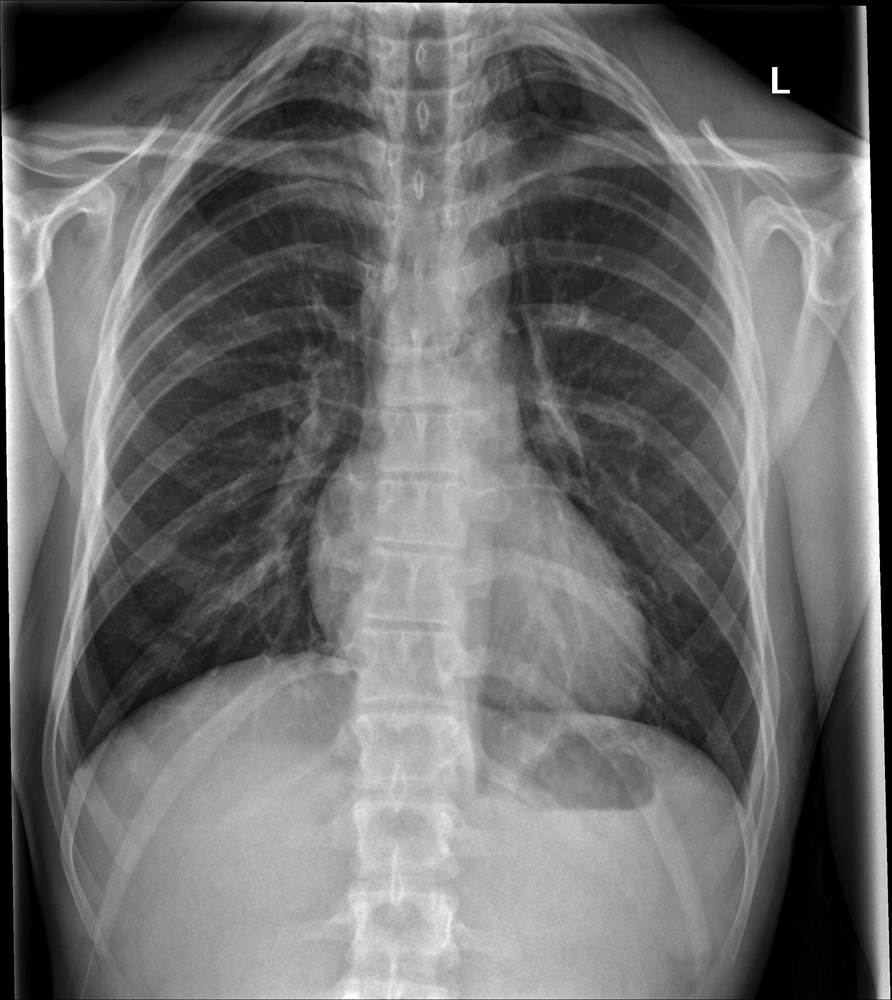
A 35 year old woman presents to ED complaining of severe sudden onset chest and epigastric pain. She has had severe vomiting and diarrhoea over the last 12 hours. Her observations are: BP 135/90, HR 110, RR 25, SpO2 96% OA. What is the most likely diagnosis?
Answer:
The x-ray shows pneumomediastinum. Effort rupture of the oesophagus (Boerhaave syndrome), is a spontaneous perforation of the oesophagus that results from a sudden increase in intraoesophageal pressure combined with negative intrathoracic pressure (e.g. severe straining or vomiting) causing a longitudinal oesophageal perforation. Findings suggestive of an oesophageal perforation on chest radiograph include mediastinal or free peritoneal air or subcutaneous emphysema. With cervical oesophageal perforations, plain films of the neck may show air in the soft tissues of the prevertebral space. Other findings suggestive of an oesophageal perforation include pleural effusions, mediastinal widening, hydrothorax, hydropneumothorax, or subdiaphragmatic air.Oesophageal Rupture
Surgical Emergencies
Last Updated: 1st February 2023
Effort rupture of the oesophagus (Boerhaave syndrome), is a spontaneous perforation of the oesophagus that results from a sudden increase in intraoesophageal pressure combined with negative intrathoracic pressure (e.g. severe straining or vomiting) causing a longitudinal oesophageal perforation. It is associated with high morbidity and mortality and is fatal in the absence of therapy. The occasionally nonspecific nature of the symptoms may contribute to a delay in diagnosis and a poor outcome. Oesophageal perforations are rare, with an incidence of 3.1 per 1,000,000 per year. Among oesophageal perforations, approximately 15 percent are spontaneous perforations.
Pathophysiology
Boerhaave syndrome usually occurs in patients with a normal underlying oesophagus. However, a subset of patients with Boerhaave syndrome has underlying eosinophilic oesophagitis, medication-induced oesophagitis, Barrett's or infectious ulcers. The oesophageal perforation usually involves the left posterolateral aspect of the distal intrathoracic oesophagus and extends for several centimeters. However, the rupture can occur in the cervical or intra-abdominal oesophagus. Rupture of the intrathoracic oesophagus results in contamination of the mediastinal cavity with gastric contents. This leads to chemical mediastinitis with mediastinal emphysema and inflammation, and subsequently bacterial infection and mediastinal necrosis. Rupture of the overlying pleura by mediastinal inflammation or by the initial perforation directly contaminates the pleural cavity, and pleural effusion results. Although pericardial tamponade and infected pericardial effusions due to Boerhaave syndrome have been reported, they are rare. If untreated, sepsis and organ failure result.
Clinical features
Boerhaave syndrome is often diagnosed incidentally in a patient being evaluated for chest pain. The diagnosis of Boerhaave syndrome should be suspected in patients with severe chest, neck, or upper abdominal pain after an episode of severe retching and vomiting or other causes of increased intrathoracic pressure, and the presence of subcutaneous emphysema on physical exam. In patients with mediastinal emphysema, mediastinal crackling with each heartbeat may be heard on auscultation especially if the patient is in the left lateral decubitus position (Hamman's sign). Within hours of the perforation, patients can develop odynophagia, dyspnea, and sepsis and have fever, tachypnea, tachycardia, cyanosis, and hypotension on physical examination. A pleural effusion may also be detected.
Diagnosis
While thoracic and cervical radiography can be supportive of the diagnosis, the diagnosis is established by contrast oesophagraphy or computed tomography (CT) scan:
- Radiography
- Findings suggestive of an oesophageal perforation on chest radiograph include mediastinal or free peritoneal air or subcutaneous emphysema. With cervical oesophageal perforations, plain films of the neck may show air in the soft tissues of the prevertebral space. Other findings suggestive of an oesophageal perforation include pleural effusions, mediastinal widening, hydrothorax, hydropneumothorax, or subdiaphragmatic air.
- Oesophageal contrast studies
- Contrast oesophagram usually establishes the diagnosis of an oesophageal perforation and reveals the location and extent of perforation by the extravasation of contrast material.
- Computed tomography
- CT scan findings consistent with an oesophageal perforation include oesophageal wall edema and thickening, perioesophageal fluid with or without gas bubbles, mediastinal widening, and air and fluid in the pleural spaces, retroperitoneum, or lesser sac.
Differential diagnosis
Patients with Mallory-Weiss syndrome may have a history of forceful retching and epigastric or back pain, but haematemesis is the major clinical manifestation. Patients with Mallory-Weiss syndrome have longitudinal mucosal lacerations in the distal oesophagus and proximal stomach and not a rupture of the oesophagus as seen in patients with Boerhaave syndrome. Patients with Mallory-Weiss syndrome therefore do not have evidence of subcutaneous, mediastinal, or peritoneal air on radiography or extravasation of oesophageal contrast on barium oesophagram/computed tomography scan.
Management
Boerhaave syndrome is rare, and there is limited evidence to guide management.
- Initial management - regardless of the subsequent management approach (medical, endoscopic, or surgical), all patients with an oesophageal perforation require the following:
- Avoidance of all oral intake
- Nutritional support, typically parenteral
- Intravenous broad spectrum antibiotic
- Intravenous proton pump inhibitor
- Drainage of fluid collections/debridement of infected and necrotic tissue, if present
- Subsequent management - management depends upon the size and location of the perforation, whether it is a contained perforation in the mediastinum or between the mediastinum and visceral lung pleura, how rapidly it is diagnosed, whether the oesophagus has underlying disease, and the patient's underlying comorbidities:
- Conservative management:
- Medical management of patients with oesophageal perforation includes the following:
- Avoidance of all oral intake for at least seven days
- Parenteral nutrition support
- Intravenous broad spectrum antibiotics for 7 to 14 days (e.g. ticarcillin-clavulanate)
- Drainage of fluid collections
- Medical management of patients with oesophageal perforation includes the following:
- Surgical management
- Patients who are not candidates for or who fail conservative attempts at treatment require surgical treatment. This can include primary repair of the defect, resection of the defect, diversion, drainage of collections, or in some cases, oesophagectomy.
- Endoscopic management
- Endoscopic treatment for an oesophageal perforation should be considered in patients with extensive underlying comorbidities who are unlikely to tolerate surgery. Endoscopic therapy should be performed provided an endoscopist who is experienced with oesophageal stent placement is available and after a discussion with a thoracic surgeon.
- Conservative management:
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |