

Surgical Emergencies
A 25 year old woman presents to the Emergency Department with a 2 day history of pain near her anus. She describes feeling an increasing swelling in the area. On examination you find a fluctuant area in the 3 o'clock perianal region with associated erythema. She is systemically well and has no past medical history. You see no evidence of fistulous disease. How should this patient be managed?
Answer:
- Surgical drainage
- The goal of treatment of anorectal abscesses is to achieve adequate drainage of the abscess without damaging the anal sphincters.
- Drainage of the abscess should be accomplished without undue delay because of the potential for the abscess to spread into a necrotising, soft-tissue infection leading to life-threatening sepsis.
- Antibiotics are not an alternative to surgical drainage of these abscesses and should be used as an adjunctive treatment.
Anorectal Abscess
Surgical Emergencies
Last Updated: 8th September 2021
An anorectal abscess is an infection of the soft tissues around the anus. For patients with Crohn's disease, an anorectal abscess will develop in approximately one third of patients. Anorectal abscesses are between 2 and 3 times more common in men than women, with most abscesses occurring in patients between 20 to 40 years of age. Anorectal abscesses are associated with anal fistulas in 37% of patients. If these fistulas are not recognised and treated, perirectal abscesses may recur.
Classification
Anorectal abscesses are usually classified clinically, based on the anatomy of the abscess.
- Intersphincteric abscesses are located in the space between the internal and external anal sphincter.
- Perianal abscesses occur in the superficial soft tissues overlying the intersphincteric space.
- Perirectal abscesses are found in the ischio-rectal or post-anal spaces.
- Supralevator abscesses occur above the anorectal ring in the supralevator space.
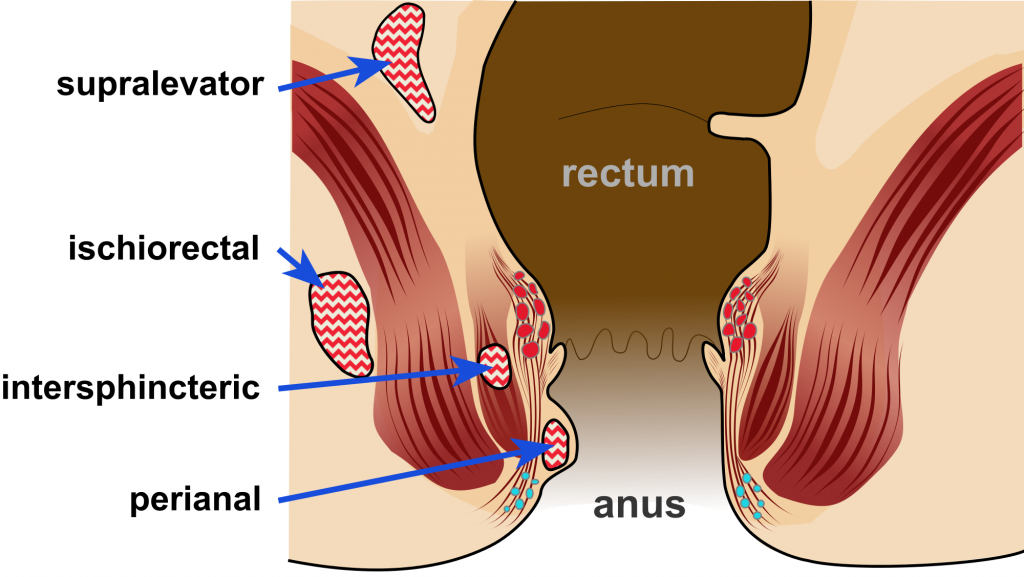
Anorectal abscess classification. (Image by McortNGHH (Own work) [CC BY-SA 4.0], via Wikimedia Commons)
Clinical features
The presence of key risk factors such as a history of Crohn's disease or anal fistula should be elicited. In addition, anorectal abscesses are more common in men than women.
Patients with anorectal abscesses usually relate a history of localised anal or perianal pain. Pain usually begins 1 to 2 days before presentation and becomes progressively more severe. Patients frequently complain of swelling and warmth of the perianal tissues. Fever is common and is usually <38.6ºC.
The most common finding on physical examination is a tender, indurated area immediately adjacent to the anus, within the anal canal, or above the anorectal ring.
Investigations
Radiological studies are rarely helpful in the diagnosis and management of anorectal abscesses. Occasionally, for patients with complex or atypical presentations, or those with supralevator or horseshoe abscesses, anal ultrasonography has been used for evaluation. However, the severe pain associated with the anorectal abscess frequently limits the use of this modality. Other imaging modalities such as CT or MRI may be more helpful in the evaluation of these patients.
Management
- Surgical drainage
- The goal of treatment of anorectal abscesses is to achieve adequate drainage of the abscess without damaging the anal sphincters.
- Drainage of the abscess should be accomplished without undue delay because of the potential for the abscess to spread into a necrotising, soft-tissue infection leading to life-threatening sepsis.
- External drainage of perianal and perirectal abscess is appropriate, while intersphincteric and supralevator abscesses should be drained internally into the anal canal and rectum, respectively, to avoid the creation of extrasphincteric or suprasphincteric fistulas.
- Adequate drainage of the abscess should result in a prompt improvement in the symptoms. If not, re-examination under anaesthesia is indicated to ensure complete drainage of the abscess.
- For patients with anorectal abscesses associated with Crohn's disease, treatment of the underlying condition should be considered after the acute anorectal sepsis has been treated.
- The management of a co-existing anal fistula should also be considered.
- Antibiotics
- Antibiotics are not an alternative to surgical drainage of these abscesses and should be used as an adjunctive treatment.
- Usually reserved for patients with diabetes, immunocompromised, chronic debilitation, older age, history of cardiac valvular disease, or significant associated cellulitis.
- Broad-spectrum antibiotics with anaerobic and gram-negative coverage should be started preoperatively and be discontinued within 24 hours of surgery or after cellulitis has resolved.
- For patients who present with a necrotising soft-tissue infection, broad-spectrum antibiotics as described above are mandatory.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |