

Infectious Diseases
An 18 month old child is brought to the Emergency Department by his parents. They describe a persistent high fever (39.5°C) and irritability over the past week. He has previously been seen by his GP who diagnosed a viral illness but his mum is worried that he has developed some skin changes. Other than his temperature, his observations are normal. On examination, you note that his lips are dry and cracked, and his tongue is enlarged, red and shiny. He has bilateral dry red eyes and tender cervical lymphadenopathy. Which of the following is the mainstay of treatment for this child's condition?
Answer:
The main goal of treatment is to prevent cardiac complications, especially coronary artery aneurysms. Other goals are to reduce the frequency and intensity of the other manifestations as early as possible. This may lead to a reduction in hospital stay and faster recovery. Standard treatment includes administering a single infusion of intravenous immunoglobulin (IVIG), early in the course of the disease within 10 days of the onset. IVIG is also indicated in patients who present after 10 days with risk factors for complications such as fever or raised acute phase markers (ESR and/or CRP). This is considered to be the most current treatment regimen and has been successful in reducing the duration of fever and the prevalence of coronary artery aneurysms in KD. Aspirin should be used with IVIG therapy and is thought to have an additive anti-inflammatory effect in KD. Low-dose aspirin should be continued for 6-8 weeks after the acute episode.Kawasaki Disease
Infectious Diseases
Last Updated: 14th December 2023
Kawasaki disease (KD) is an acute, febrile, self-limiting, systemic vasculitis of unknown origin that almost exclusively affects young children, with peak incidence between the ages of 13-24 months. KD occurs more often in males than in females (1.5:1). Although a human leukocyte antigen (HLA) association has not yet been identified, the incidence of KD is significantly increased in Japan and Korea, as well as among Asian-American children in the US. In an immunogenetically predisposed host, one or more infectious agents may play a role in triggering the clinical manifestations of the disease.
Clinical features
Diagnostic features of classic KD:
Fever (>39°C) lasting longer than 5 days, marked irritability of the child and at least 4 of the following:
- Non-purulent bilateral conjunctival injection
- Polymorphous erythematous rash
- Cervical lymphadenopathy, usually unilaterally
- Oropharyngeal changes, including diffuse hyperaemia, strawberry tongue, and lip changes (e.g. swelling, fissuring, erythema, and bleeding)
- Peripheral extremity changes, including erythema, oedema, induration, and desquamation, which may cause difficulty walking
Less common findings may include: stiff neck secondary to aseptic meningitis, facial palsy, anterior uveitis (70%), pleural effusion, pulmonary infiltrates, pericardial effusion with or without myocarditis, and congestive heart failure.
Others include: abdominal pain, diarrhoea, hepatitis, obstructive jaundice, gallbladder distension or hydrops of the gallbladder, pancreatitis, joint involvement (arthralgias or arthritis), meatitis, vulvitis, urethritis with sterile pyuria, proteinuria, nephritis, and acute renal failure. In addition, peripheral extremity gangrene, pustules, erythema multiforme-like lesions, perianal erythema (50% to 70%), macules, papules, measles-like rash, and scarlet fever-like erythema may be found.
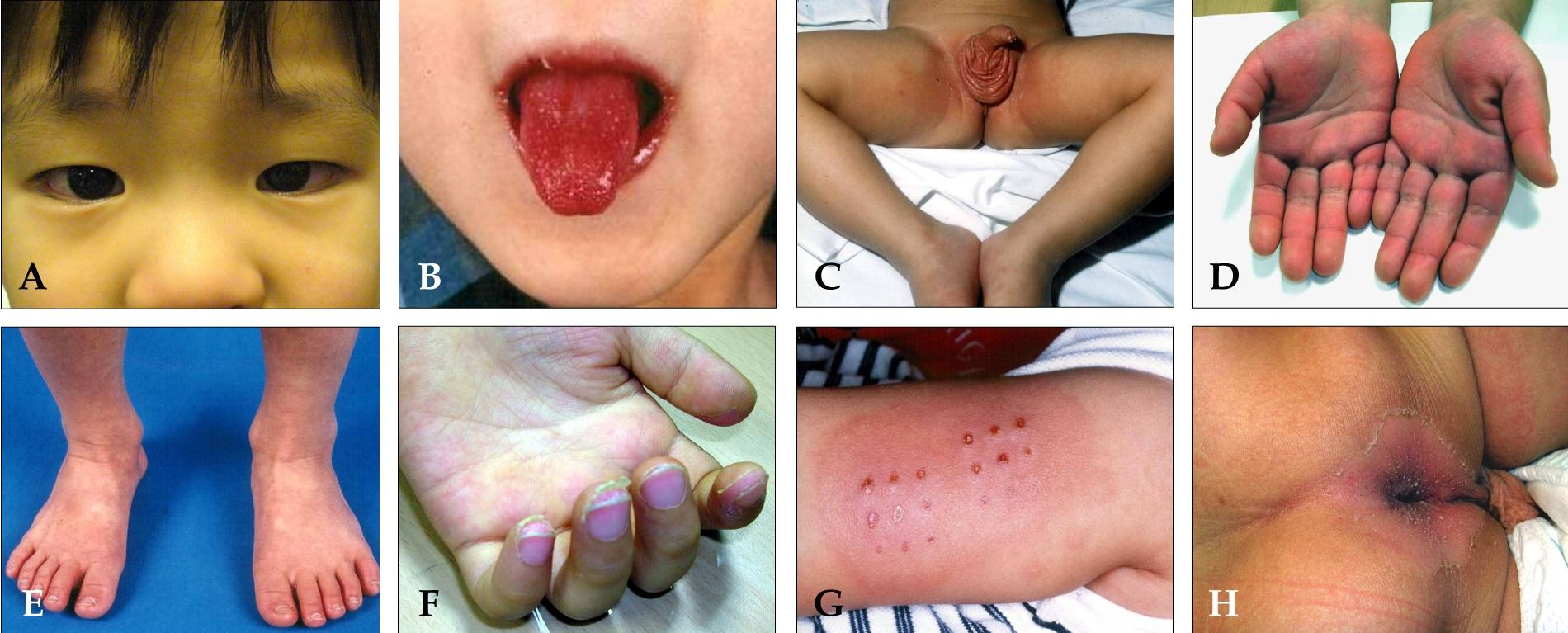
Clinical features of Kawasaki disease. (Image by Dong Soo Kim (Kawasaki disease.) [CC BY-SA 4.0 , via Wikimedia Commons)
- (A) Bilateral, non-exudative conjunctival injection with perilimbal sparing
- (B) Strawberry tongue and bright red, swollen lips with vertical cracking and bleeding
- (C) Erythematous rash involving perineum
- (D) Erythema of the palms, which is often accompanied by painful, brawny oedema of the dorsa of the hands
- (E) Erythema of the soles, and swelling dorsa of the feet
- (F) Desquamation of the fingers
- (G) Erythema and induration at the site of a previous vaccination with Bacille Calmette-Guerin (BCG)
- (H) Perianal erythematous desquamation
Investigations
Diagnosis is based on clinical signs and symptoms. There are no unique laboratory diagnostic tests for the disease.
The presence of three or more of the following laboratory features may increase the index of suspicion for KD:
- Anaemia
- Platelet count of > 450,000 after day 7 of fever
- Albumin < 3.0 g/dL
- Elevated alanine aminotransferase (ALT)
- White blood cell (WBC) count > 15,000
- Urine with > 10 WBC/high power field.
Some laboratory tests may be supportive, such as acute phase reactants, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). These are significantly raised (to a greater degree than that found in common viral infections).
Because coronary artery aneurysms are the hallmark of KD, perform echocardiography at diagnosis and routinely repeat it at 1-2 weeks and 4-6 weeks after treatment. If coronary artery abnormalities are significant (Z score >2.5) during the acute illness, perform echocardiography at least twice per week until luminal dimensions have stopped progressing. Be aware that in the first week of illness, the echocardiogram is typically normal and does not rule out the diagnosis. If the echocardiographic findings are abnormal at any stage in the course of the illness, refer the patient a paediatric cardiologist for a complete cardiac work-up and follow-up care.
Clinical stages
- Acute febrile stage (lasting weeks 1-2)
- Fever, irritability, cervical adenitis, conjunctivitis, rash, mucosal erythema, painful erythema of the hands and feet, arthralgia or arthritis, possible myocarditis, and pericarditis.
- Subacute stage (lasting weeks 2-4)
- Fever, rash, and lymphadenopathy have resolved; if fever persists there is an increased risk of cardiac complications; persistent irritability, poor appetite, and conjunctival injection; desquamation of extremities begins at this stage. Cardiac abnormalities (coronary artery ectasia or aneurysms) may develop during this stage.
- Convalescent stage (lasting weeks 4-8)
- All signs of inflammation have receded and acute phase markers normalise. If present, coronary artery ectasia or aneurysms may persist and enlarge.
- Chronic stage (variable)
- If present, coronary artery dilation may resolve. However, coronary artery aneurysms may persist through adulthood. Such patients are at risk of subsequent coronary artery thrombosis, rupture, and myocardial infarction.
Differential diagnosis
- Staphylococcal or streptococcal infection
- Systemic juvenile idiopathic arthritis (systemic JIA)
- Scarlet fever
- Acute rheumatic fever
- Toxic shock syndrome (TSS)
- Staphylococcal scalded skin syndrome
- Stevens-Johnson syndrome
- Drug reaction
- Rocky Mountain spotted fever
- Measles
Management
The main goal of treatment is to prevent cardiac complications, especially coronary artery aneurysms. Other goals are to reduce the frequency and intensity of the other manifestations as early as possible. This may lead to a reduction in hospital stay and faster recovery.
Standard treatment includes administering a single infusion of intravenous immunoglobulin (IVIG), early in the course of the disease within 10 days of the onset. IVIG is also indicated in patients who present after 10 days with risk factors for complications such as fever or raised acute phase markers (ESR and/or CRP). This is considered to be the most current treatment regimen and has been successful in reducing the duration of fever and the prevalence of coronary artery aneurysms in KD. Aspirin should be used with IVIG therapy and is thought to have an additive anti-inflammatory effect in KD. Low-dose aspirin should be continued for 6-8 weeks after the acute episode. Corticosteroids and other immunosuppressive therapies or very rarely, plasma exchange may be considered in refractory KD.
Patients with KD that present after day 10 without persistent fever, and when their acute phase markers (ESR and/or CRP) are normal, are regarded as without risk of developing coronary aneurysms. If their initial and subsequent echocardiograms are normal, they should be treated with low-dose aspirin until 6-8 weeks from the onset. If echocardiogram at 8 weeks is normal, low-dose aspirin can be discontinued. However, if diagnosed after day 10 with evidence of elevated ESR or CRP and/or coronary abnormalities on echocardiogram, patients should be treated as detailed above for patients with risk factors for complications.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |